Jessica James, Contributing Writer08.08.17
Accurate placement of the acetabular component during total hip arthroplasty (THA) is an important factor in the success of the procedure. New software tools and pre-surgical planning guides are being developed to improve surgical outcomes and reduce the risks associated with component malorientation. The Corin Group in Australia have recently enjoyed success with its Optimized Positioning System (OPS) technology, which uses image-based modeling techniques through Simpleware software (Synopsys, Mountain View, Calif.) to solve key challenges in patient-specific simulation and hip replacements.
By using a combination of imaging protocols, simulation, and 3D printing, this technology is extending the options available to surgeons when planning total hip replacements. The ability to accurately predict and reduce the margin of error associated with implant orientation and hip biomechanics is particularly valuable, in this context, for surgical decision-making and improving the outcomes for patients with different needs. How, then, does this patient-specific simulation technology solve some of the longer-term challenges of optimizing total hip replacements?
Pre-Surgical Planning: Growth Trends
Virtual surgical planning is becoming increasingly common within the orthopedic sector, from improving the chance of positive outcomes for knee and hip replacements, through to enhancing techniques for different surgical procedures. The latest techniques typically bring together a range of technologies, including 3D imaging, model generation and simulation software, 3D printing, and robot and laser-assisted instrumentation. The use of computational simulation and 3D printing in surgical planning is also gaining traction with the FDA, albeit with a continuing need for extensive verification, validation, and clinical testing prior to application; these concerns are particularly important for regulatory decisions involving software interfaces with physical medical devices and instrumentation.
The potential long-term benefits to surgeons of new technologies for procedure planning and decision-making are clear: improved accuracy, a smaller risk of misalignment and infection, as well as a reduced need for revision surgeries. These trends also align with patient customization using additive manufacturing to tailor implants. Meeting the demands of patient variability while ensuring quality implants and repeatability was one of the key challenges for Corin in developing the OPS System.
Challenges
Optimal orientation of the acetabular component in THA is traditionally planned by using “safe zones” defined from the literature. These zones typically prescribe generic targets of 35o to 45o of inclination, and 5o to 25o of anteversion. However, these figures are not exact, and it is difficult to arrive at a definite reference point for a specific patient anatomy. Pelvic tilt is also an important factor when evaluating a patient’s physiological profile, whereby the arc of pelvic motion can be as much as 70o for some patients,1 and for others as stiff as 5o.2 Not taking this into account during surgical planning can make a significant difference to the functional performance of the acetabular cup. The use of safe zones is consequently being challenged as a method for deciding on the optimal placement of acetabular components.3-5
Clinical research indicates that up to 50 percent of hip surgeries miss their intended orientation,6 while the success rate can be as low as 21.5 percent.7 An inaccurate cup orientation increases the risk of dislocation, surface wear, squeaking, and many other problems that can negatively impact upon patient comfort and the long-term success of the implant. Generic zones of movement do not always apply, creating a need to design an orientation that is suitable to the specific patient. In attempting to achieve these optimized outcomes, orthopedic surgeons traditionally use an AP (anterior-posterior) X-ray scan of patients to plan a specific implant arrangement, and to approximate the size of the implant needed for the surgery. These approximations are still limited, though, by working on a 2D plane, making it difficult to properly visualize and predict results.
The goal of the work carried out by Corin in developing the OPS tool was therefore focused on two key areas: first, defining where to place the acetabular component on a patient specific basis and second, achieving this target orientation in the operating room. To achieve this goal, it was necessary to create a simple but effective system for going from patient scans through to accurate computational and physical models suitable for planning and executing total hip arthroplasty surgeries.
Creating a Complete Solution
The Corin OPS system begins with 3D images of patient anatomies, obtained from computed tomography and X-ray tomography scans. This data is then imported to Simpleware software for segmentation into regions of interest for simulation. Landmarks are taken on each patient’s skeleton to identify implant placement on bones. Completing this process is often laborious and time-consuming, particularly when working with large amounts of image data.
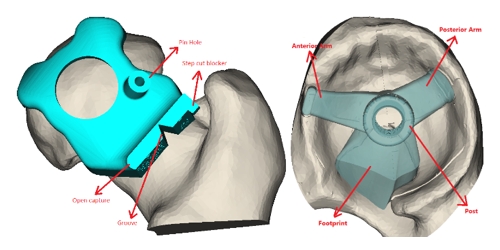
Figure 1: Analysis of CAD and anatomical models
To solve these problems, Corin engineers used the 3D visualization tools in Simpleware software to more easily understand optimal placements, speeding up the analysis process compared to traditional 2D X-ray-based templating. Scripting tools and routines were also implemented within Simpleware to reduce the amount of time spent working with similar sets of data, and to generate computer models quickly and accurately. Models are then simulated within the OPS system to analyze different types of movement and orientation, as well as a patient’s physiological profile during various daily activities. The extensive simulation studies used in designing the OPS tool involved optimally orientating the cup within a safe zone, and maintaining that position as the pelvis rotates throughout functional activity.
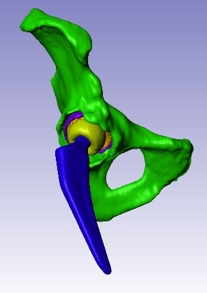
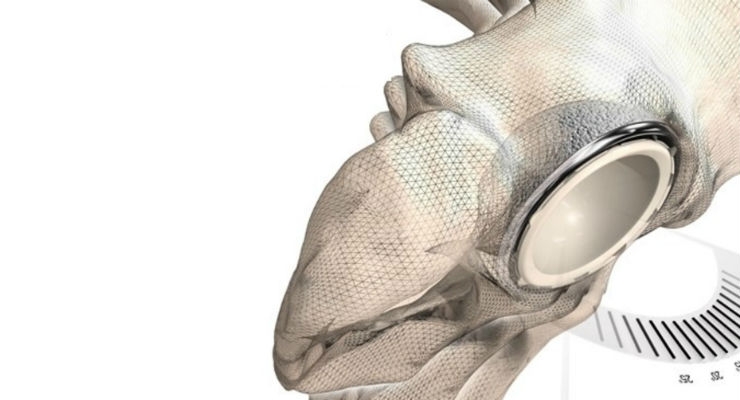
Figure 2: Modeling of hip implants
These anatomical models are combined with computer-aided design (CAD) implant geometries, which are fitted to an individual patient’s CT reference frame to measure and virtually experiment with optimal positions. From these models, 3D-printed guides are created to assist in procedures. Intended orientations are designed into the axis of the guide, with surgeons relying on the accuracy of the computer models from scan to simulation to create a secure fit to the patient’s bones, and to achieve positive intraoperative results. Being able to work with both CAD models and models created from 3D image data in Simpleware has many advantages, most notably being able to see how different designs interact with a patient-specific anatomy.
The guides created for the individual patient are used during surgery with a laser-guided alignment system to achieve an exact fit to the optimized requirements and reference markings indicated by the planning stage. Specific care is taken to maintain the correct laser alignment during the cup impaction process and confirmation of orientation, assisted by the reference markings on the acetabular model. An electronic report is also used for additional visual confirmation.

Figure 3: 3D printed models
Clinical Applications
OPS has been the subject of ongoing clinical evaluation with results being reported in peer reviewed literature. One recent study, carried out between June and September 2015, showed that accurate placement of the acetabular component can be achieved using these patient specific guides. In 91 percent of cases, the patient-specific target of ±10° was achieved for both inclination and anteversion. The accuracy of the system was demonstrated to be superior to free hand methods and comparable to navigated and robotic techniques. The study also showed a negligible increase in intra-operative time: the pre-operative stage lasted approximately three weeks, with the potential to be sped up. Aside from the cost of pre-operative CT scans, it was found that there were no additional direct costs for patients and physicians for using the system, beyond that which is typically incurred by the implant.
Following extensive use in Europe and Australia, the initial launch of the technology in the United States took place in summer 2016, beginning with early evaluations by surgeons and building toward its first use in operations in November 2016. Over one hundred OPS procedures have now been successfully performed, and patient outcomes so far have been good. Dr. Michael Swank of the Cincinnati Orthopaedic Research Institute particularly noted that “the planning was awesome."8 The technology is also being used at institutions such as the Orthopaedic Specialty Institute in Orange County, South County Orthopaedics in Wakefield, New York Orthopaedics, Inv08 Orthopaedics in Houston, and the NYU Hospital for Joint Disease. Ninety percent of the evaluator surgeons described how the new system led them to orient the acetabular component in a different position than initially planned. The OPS system has also been recognized by Good Design Awards in 2015 and 2016 and recently received FDA 510(k) clearance in the United States.
Conclusions, Future Challenges, and Opportunities
The OPS system was developed as a way of enhancing the options available to surgeons working on total hip replacements, tackling the traditional problem of achieving a “safe zone” for implant position when designing solutions for individual patients. The use of 3D image-based modeling tools in Simpleware enabled the complexities of a patient anatomy to be quickly and accurately reproduced and used as the basis for testing out different simulated positions.
There are still some challenges involved in using this technology, however, including having to account for certain patient conditions that do not lend themselves well to the procedures and methods involved. These contraindications include situations where total hip arthroplasty is not suitable for the patient, and where they might have orthopedic deformities, insufficient bone structure of quality, or obesity levels that compromise the ability of the surgeon to use the techniques effectively.
The advances made by OPS in pre-surgical planning, however, demonstrates how these complete workflows can save surgeons time and manual effort when designing medical devices and the details of particular procedures. Future improvements to the system might include increases in the amount of image segmentation tasks that can be automated, allowing for more detailed planning. The long-term success rate of the techniques used will also require continued clinical evaluation, as will advances in the types of hip implants that can be used, extending the amount of choice available for tailoring implants to patients.
The workflow used by OPS has applications in other surgical procedures (e.g., in planning for knee replacements). With computational modeling becoming more of a standard for orthopedic surgeries, the applications to making surgical plans as realistic as possible can extend to virtual reality and the production of very precise implants that consider small differences in the needs of an individual patient and the chosen implant.
References
1 DiGioia AM, Hafez MA, Jaramaz B, Levison TJ, Moody JE, Functional pelvic orientation measured from lateral standing and sitting radiographs. Clin Orthop Relat Res 453:272–276.
2 SA, Yeung E, Jackson MP, Rajaratnam S, Martell JM, Walter WL, Zicat BA, Walter WK. The role of patient factors and implant position in squeaking of ceramic-on-ceramic total hip replacements. J Bone Joint Surg 2011; Apr: 93-B;4.
3 Yoon Y, Hodgson AJ, Tonetti J, et al. Resolving inconsistencies in defining the target orientation for the acetabular cup angles in total hip arthroplasty. Clin Biomech 2008; 23:253.
4 McCollum DE, Gray WJ. Dislocation after total hip arthroplasty. Causes and prevention. Clin Orthop Relat Res 1990; 261:159.
5 Harris W. Advances in surgical technique for total hip replacement: without and with osteotomy of the greater trochanter. Clin Orthop Relat Res 1990; 146:188.
6 Callanan MC, Jarrett B, Bragdon CR, Zurakowski D, Rubash HE, Freiberg AA, Malchau H. Risk factors for cup malpositioning quality improvement through a joint registry at a tertiary hospital. Clin Orthop Relat Res 2011; 469:319–329.
7 Bosker BH, Verheyen CCPM, Horstmann WG, Tulp NJA. Poor accuracy of freehand cup positioning during total hip arthroplasty. Arch Orthop Trauma Surg 2007; 127:375–379.
8 Anon. Successful Phase 1 launch of OPSTM in the USA, Articul News 2017; 5:10-11.
Jessica James, Ph.D., works on marketing for Simpleware, a Synopsys software product. She is involved in developing awareness of 3D image-based modeling for orthopedics and other applications. She received her Ph.D. from the University of Exeter, and can be reached at simpleware@synopsys.com.
By using a combination of imaging protocols, simulation, and 3D printing, this technology is extending the options available to surgeons when planning total hip replacements. The ability to accurately predict and reduce the margin of error associated with implant orientation and hip biomechanics is particularly valuable, in this context, for surgical decision-making and improving the outcomes for patients with different needs. How, then, does this patient-specific simulation technology solve some of the longer-term challenges of optimizing total hip replacements?
Pre-Surgical Planning: Growth Trends
Virtual surgical planning is becoming increasingly common within the orthopedic sector, from improving the chance of positive outcomes for knee and hip replacements, through to enhancing techniques for different surgical procedures. The latest techniques typically bring together a range of technologies, including 3D imaging, model generation and simulation software, 3D printing, and robot and laser-assisted instrumentation. The use of computational simulation and 3D printing in surgical planning is also gaining traction with the FDA, albeit with a continuing need for extensive verification, validation, and clinical testing prior to application; these concerns are particularly important for regulatory decisions involving software interfaces with physical medical devices and instrumentation.
The potential long-term benefits to surgeons of new technologies for procedure planning and decision-making are clear: improved accuracy, a smaller risk of misalignment and infection, as well as a reduced need for revision surgeries. These trends also align with patient customization using additive manufacturing to tailor implants. Meeting the demands of patient variability while ensuring quality implants and repeatability was one of the key challenges for Corin in developing the OPS System.
Challenges
Optimal orientation of the acetabular component in THA is traditionally planned by using “safe zones” defined from the literature. These zones typically prescribe generic targets of 35o to 45o of inclination, and 5o to 25o of anteversion. However, these figures are not exact, and it is difficult to arrive at a definite reference point for a specific patient anatomy. Pelvic tilt is also an important factor when evaluating a patient’s physiological profile, whereby the arc of pelvic motion can be as much as 70o for some patients,1 and for others as stiff as 5o.2 Not taking this into account during surgical planning can make a significant difference to the functional performance of the acetabular cup. The use of safe zones is consequently being challenged as a method for deciding on the optimal placement of acetabular components.3-5
Clinical research indicates that up to 50 percent of hip surgeries miss their intended orientation,6 while the success rate can be as low as 21.5 percent.7 An inaccurate cup orientation increases the risk of dislocation, surface wear, squeaking, and many other problems that can negatively impact upon patient comfort and the long-term success of the implant. Generic zones of movement do not always apply, creating a need to design an orientation that is suitable to the specific patient. In attempting to achieve these optimized outcomes, orthopedic surgeons traditionally use an AP (anterior-posterior) X-ray scan of patients to plan a specific implant arrangement, and to approximate the size of the implant needed for the surgery. These approximations are still limited, though, by working on a 2D plane, making it difficult to properly visualize and predict results.
The goal of the work carried out by Corin in developing the OPS tool was therefore focused on two key areas: first, defining where to place the acetabular component on a patient specific basis and second, achieving this target orientation in the operating room. To achieve this goal, it was necessary to create a simple but effective system for going from patient scans through to accurate computational and physical models suitable for planning and executing total hip arthroplasty surgeries.
Creating a Complete Solution
The Corin OPS system begins with 3D images of patient anatomies, obtained from computed tomography and X-ray tomography scans. This data is then imported to Simpleware software for segmentation into regions of interest for simulation. Landmarks are taken on each patient’s skeleton to identify implant placement on bones. Completing this process is often laborious and time-consuming, particularly when working with large amounts of image data.
Figure 1: Analysis of CAD and anatomical models
Figure 2: Modeling of hip implants
The guides created for the individual patient are used during surgery with a laser-guided alignment system to achieve an exact fit to the optimized requirements and reference markings indicated by the planning stage. Specific care is taken to maintain the correct laser alignment during the cup impaction process and confirmation of orientation, assisted by the reference markings on the acetabular model. An electronic report is also used for additional visual confirmation.
Figure 3: 3D printed models
OPS has been the subject of ongoing clinical evaluation with results being reported in peer reviewed literature. One recent study, carried out between June and September 2015, showed that accurate placement of the acetabular component can be achieved using these patient specific guides. In 91 percent of cases, the patient-specific target of ±10° was achieved for both inclination and anteversion. The accuracy of the system was demonstrated to be superior to free hand methods and comparable to navigated and robotic techniques. The study also showed a negligible increase in intra-operative time: the pre-operative stage lasted approximately three weeks, with the potential to be sped up. Aside from the cost of pre-operative CT scans, it was found that there were no additional direct costs for patients and physicians for using the system, beyond that which is typically incurred by the implant.
Following extensive use in Europe and Australia, the initial launch of the technology in the United States took place in summer 2016, beginning with early evaluations by surgeons and building toward its first use in operations in November 2016. Over one hundred OPS procedures have now been successfully performed, and patient outcomes so far have been good. Dr. Michael Swank of the Cincinnati Orthopaedic Research Institute particularly noted that “the planning was awesome."8 The technology is also being used at institutions such as the Orthopaedic Specialty Institute in Orange County, South County Orthopaedics in Wakefield, New York Orthopaedics, Inv08 Orthopaedics in Houston, and the NYU Hospital for Joint Disease. Ninety percent of the evaluator surgeons described how the new system led them to orient the acetabular component in a different position than initially planned. The OPS system has also been recognized by Good Design Awards in 2015 and 2016 and recently received FDA 510(k) clearance in the United States.
Conclusions, Future Challenges, and Opportunities
The OPS system was developed as a way of enhancing the options available to surgeons working on total hip replacements, tackling the traditional problem of achieving a “safe zone” for implant position when designing solutions for individual patients. The use of 3D image-based modeling tools in Simpleware enabled the complexities of a patient anatomy to be quickly and accurately reproduced and used as the basis for testing out different simulated positions.
There are still some challenges involved in using this technology, however, including having to account for certain patient conditions that do not lend themselves well to the procedures and methods involved. These contraindications include situations where total hip arthroplasty is not suitable for the patient, and where they might have orthopedic deformities, insufficient bone structure of quality, or obesity levels that compromise the ability of the surgeon to use the techniques effectively.
The advances made by OPS in pre-surgical planning, however, demonstrates how these complete workflows can save surgeons time and manual effort when designing medical devices and the details of particular procedures. Future improvements to the system might include increases in the amount of image segmentation tasks that can be automated, allowing for more detailed planning. The long-term success rate of the techniques used will also require continued clinical evaluation, as will advances in the types of hip implants that can be used, extending the amount of choice available for tailoring implants to patients.
The workflow used by OPS has applications in other surgical procedures (e.g., in planning for knee replacements). With computational modeling becoming more of a standard for orthopedic surgeries, the applications to making surgical plans as realistic as possible can extend to virtual reality and the production of very precise implants that consider small differences in the needs of an individual patient and the chosen implant.
References
1 DiGioia AM, Hafez MA, Jaramaz B, Levison TJ, Moody JE, Functional pelvic orientation measured from lateral standing and sitting radiographs. Clin Orthop Relat Res 453:272–276.
2 SA, Yeung E, Jackson MP, Rajaratnam S, Martell JM, Walter WL, Zicat BA, Walter WK. The role of patient factors and implant position in squeaking of ceramic-on-ceramic total hip replacements. J Bone Joint Surg 2011; Apr: 93-B;4.
3 Yoon Y, Hodgson AJ, Tonetti J, et al. Resolving inconsistencies in defining the target orientation for the acetabular cup angles in total hip arthroplasty. Clin Biomech 2008; 23:253.
4 McCollum DE, Gray WJ. Dislocation after total hip arthroplasty. Causes and prevention. Clin Orthop Relat Res 1990; 261:159.
5 Harris W. Advances in surgical technique for total hip replacement: without and with osteotomy of the greater trochanter. Clin Orthop Relat Res 1990; 146:188.
6 Callanan MC, Jarrett B, Bragdon CR, Zurakowski D, Rubash HE, Freiberg AA, Malchau H. Risk factors for cup malpositioning quality improvement through a joint registry at a tertiary hospital. Clin Orthop Relat Res 2011; 469:319–329.
7 Bosker BH, Verheyen CCPM, Horstmann WG, Tulp NJA. Poor accuracy of freehand cup positioning during total hip arthroplasty. Arch Orthop Trauma Surg 2007; 127:375–379.
8 Anon. Successful Phase 1 launch of OPSTM in the USA, Articul News 2017; 5:10-11.
Jessica James, Ph.D., works on marketing for Simpleware, a Synopsys software product. She is involved in developing awareness of 3D image-based modeling for orthopedics and other applications. She received her Ph.D. from the University of Exeter, and can be reached at simpleware@synopsys.com.