10.01.08
Material Marvels
Titanium is a top choice for implants, but other materials are gaining popularity.
Michael Barbella
Craig Schank considers his job to be a simple one: He fulfills a need to the medical device industry.
During the past 25 years, however, Schank’s job has become more complicated as medical device manufacturers—particularly those that produce orthopedic implants—discovered the benefits of titanium. “I’ve been selling titanium to this market since 1982-1983, and over the years, the need has just gotten stronger and stronger,” he noted. “It’s been a challenge over the years to keep the metal on the shelf. The spinal industry used to use stainless steel almost exclusively; now they use titanium almost exclusively.”
The switch, however, did not happen overnight. Schank still can remember the disdain he encountered from the spinal implant industry when he first inquired about using titanium for the devices.
“I remember walking into a spinal [implant] company in the late 1980s to introduce titanium to them, because they were still using stainless steel. Most of the spinal companies used only stainless steel back then,” recounted Schank, director of sales and marketing for Supra Alloys, a titanium service provider based in Camarillo, CA. “And the guy at this company said to me, ‘I can tell you we will never use titanium.’”
That edict proved to be short-lived, as the demand for orthopedic implants began to rise and implant manufacturers looked for materials that would provide greater durability and more flexibility. In the two decades since Schank encountered his first rebuff of the material, titanium has replaced stainless steel as the metal of choice among orthopedic implant manufacturers.
There are many reasons for titanium’s popularity, but suppliers who spoke with Orthopedic Design & Technology said one of the main factors is its natural properties. Not only does titanium have the highest strength-to-density ratio of any metal, suppliers said, it essentially is non-magnetic and highly resistant to corrosion. In addition, titanium weighs less than most other alloys, transfers heat well, has a higher melting point than steel and is nontoxic and biologically compatible with human bones and tissue, making it an ideal material for orthopedic implants.
It is titanium’s durability, however, that has made it a popular choice among manufacturers of hip, knee and spinal implants. With baby boomers leading more active lifestyles and young athletes sustaining season-ending (if not career-ending) injuries, manufacturers have had to find materials that would extend the lifespan of joint implants.
“The procedures [doctors] are performing today they are performing on younger people, and the materials are better, stronger and last a longer period of time,” said William Keaveney, sales manager at Boston Centerless, a supplier of precision ground bar stock based in Woburn, MA. “In years past, say 20 or 30 years ago, when doctors performed a hip replacement, they performed it on someone who was older. Today, they do hip replacements on people who are 50 years old or even younger, so the implant has to be made out of something that is going to last. These people still want to lead an active life—they still want to go out and play golf.”
Research suggests that legions of older Americans are going to want to go out and play golf in the coming decades. A study by Exponent Inc., an engineering and scientific consulting firm based in Menlo Park, CA, concluded that the number of first-time total knee replacements would skyrocket 673% by 2030 while the number of primary hip replacements would jump 175%.
With such a high demand projected for the future, titanium (and titanium alloys) easily should remain a top material choice among implant manufacturers, suppliers said. Companies also are working on developing new grades of the metal in an effort to boost its functionality.
During the past quarter century, titanium has become the metal of choice among orthopedic implant manufacturers. Photo courtesy of Supra Alloys. |
“We are seeing increasing demand for customized alloys and product forms that have to be tailored specifically to satisfy surgeon preferences,” reported Michael J. Walter, medical market development manager for Carpenter Technology.
In addition to its Micro-Melt product line and BioDur 108, Carpenter manufactures BioDur CCM Plus Alloy, a metal that offers improved wear resistance, finer grain and enhanced forgeability; SLIC titanium for formed fasteners made from pre-straightened coil; titanium ULTRABAR; and Ti15Mo, which can achieve higher properties, depending on the application.
Besides the innovative materials manufactured by companies such as Carpenter, recent advances in science and technology promise to bring a host of new materials to the market in the near future. Last fall, for example, engineers from Brown University in Providence, RI revealed that they had discovered a new material that helps bone-forming cells grow faster and meld better to the metal in artificial hips, knees and shoulders. The new material was composed of carbon nanotubes on anodized titanium.
The team took titanium, chemically treated it and applied an electrical current to it, according to the university. The process, called anodization, created a pitted coating in the surface of the titanium. The team then packed those pits with a cobalt catalyst and heated the samples to 700 degrees Celsius. The process caused carbon nanotubes to sprout from each pit.
Engineers placed human bone-forming cells onto the nanotube-covered samples as well as onto samples of plain and anodized titanium. The samples were placed in an incubator; after three weeks, engineers discovered that the bone cells grew twice as fast on the titanium covered in nanotubes.
“What we found is possibly a new material for joint replacement and other implants,” said Thomas Webster, an associate engineering professor at Brown University. “Right now, bone doesn’t always properly meld to implants. Osteoblasts don’t grow or grow fast enough. Adding carbon nanotubes to anodized titanium appears to encourage that cell growth and function.”
Several months after the engineers’ discovery was announced, DePuy Orthopaedics Inc.’s Gription Porous Coating received 510(k) clearance from the FDA for use on the Warsaw, IN-based company’s Pinnacle Acetabular Cup System. The coating, composed of a titanium alloy structure, contains a high coefficient of friction and an engineered porous surface that features 63% porosity and a 300-micron average pore size. The coating, according to the company, has a sandpaper-like surface that covers the implant with pores and creates a rough surface that helps the bone grip with the implant.
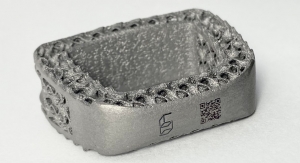
And in May, Arcam EBM, a high-tech company based in Gothenburg, Sweden that provides implant manufacturers with machines for titanium and cobalt chrome alloys, introduced a new form of titanium for the production of orthopedic implants. The company developed Titanium Grade 2 (ASTM F67, unalloyed titanium) to produce orthopedic implants with integrated lattice structures for improved bone in-growth.
Implants produced with Arcam’s EBM (electron beam melting) technology are built up layer by layer from metal powder melted with an electron beam gun inside a vacuum chamber, according to the company. The EBM machines manufacture implants with integrated lattice facades that enhance the adherence of bone to the implant surface.
Nitinol and Other Materials
Titanium’s biocompatibility and durability have helped make it a favorite material for use in orthopedic implants. However, manufacturers haven’t completely abandoned other metals.
Most hip and knee implants are made partially of cobalt-chromium alloys (see the sidebar, “Critical Components of Total Hip and Knee Replacements”), while stainless steel remains the material of choice for surgical instruments because it is strong, durable and able to withstand harsh sterilization procedures.
“Cobalt/chromium/molybdenum is an alloy that is used for certain implantable applications. It is used mostly for things that go into the body and stay there,” Keaveney noted. “Then there are other alloys used for medical devices. There is 440A and 440C stainless steel, 17-4PH (Custom 630) stainless steel, and a number of similar grades that are used for applications outside of the body. The materials used today are stronger and more durable. Of course, we’re putting more demands on the implants, too. If you are putting a new hip in a 50-year-old man as opposed to a 75-year-old man, the implant has to be more durable.”
Other materials are being incorporated into orthopedic devices as well. Nickel titanium, an alloy better known as nitinol (named after its place of discovery—Nickel Titanium Naval Ordinance Laboratory), is gaining popularity among OEMs for its unique mechanical properties—super elasticity and shape memory—and good biocompatibility.
Nitinol, if deformed while it is cool, returns to its original shape when it is warmed. According to research, nitinol and copper-based alloys have been found to recover substantial amounts of strain, and/or generate significant force, when changing shape.
Titanium isn't the only material used for orthopedic implants. Also popular are precision-ground metals and polyethylene, one of the most common materials in implants. Photo courtesy of Boston Centerless. |
Fort Wayne Metals manufactures three medical grades of nitinol wire products. The firm produces precision ground rod and bar products available in diameters ranging from 0.071 to 0.250 inch, with some alloys ranging up to 0.3937 inch. The wire is used in spinal rods, bone pins and screws, nails, spinal devices, cerclage cables, guide rods and reamer rods.
BioMedical Enterprises Inc., a 17-year-old medical device company in San Antonio, TX, has developed a nitinol implant called OSSArc that conforms to sloping and irregular bone surfaces. The implant, according to the company, is ideal for procedures such as Akin osteotomies, fractures of the fifth metatarsal in the foot and metacarpal fractures in the hand.
With an eye toward the future, researchers in England are experimenting with a porous glass implant that dissolves in the body and releases calcium that encourages damaged bones to regrow. Currently in development at Imperial College in London, with the Universities of Kent and Warwick, the implant is designed to act as a replacement for missing bone.
According to published reports, the implant is composed of clouded glass containing honeycomb-like pores that resemble the inner layer of bone. The pores contain calcium. Once in place, the implant reacts with bodily fluids and gradually dissolves, bonding to existing bone and creating a scaffold for new bone to grow, the reports said. The implant dissolves at the same rate the new bone grows and releases other elements such as silicon, which stimulates the body’s bone growth cells.
The implant would be available in various shapes and sizes, depending on where it was needed.
The Power of Polymers: Polyethylene and PEEK
Polyethylene is another one of the most commonly used materials in orthopedic implants. The durable plastic—ideal for joint replacements—is used mostly on the surface of one implant to contact another implant.
Polyethylene shares some of the same properties as titanium—namely durability, biocompatibility and strength. These qualities have helped make it a popular choice among younger implant recipients, particularly since polyethylene implants can be made more resistant to wear through a process called cross-linking. This process creates stronger bonds between the elements that comprise the polyethylene.
“Plastics are being used more and more in the orthopedic industry,” Keaveney noted. “There are a number of plastics called medical-grade plastics that are tough, durable, and processed to be implanted in the body. It’s a growing part of the industry.”
One type of polymer that suppliers said is becoming the material of choice for orthopedic implant applications is polyetheretherketone, or PEEK. This type of polymer exhibits a combination of strength, stiffness and toughness, is biocompatible and can be repeatedly sterilized without losing any of its mechanical properties. In addition, PEEK is hypo-allergenic and non-magnetic, enabling patients who have received implants made with this material to undergo procedures such as magnetic resonance imaging.
Invibio Biomaterial Solutions, a West Conshohocken, PA-based company that provides medical device manufacturers with implantable PEEK polymers, is working with orthopedic giant Smith & Nephew to develop a line of structural bioresorbable polymers. The companies hope to create advanced structural bioresorbable materials with the performance specifications needed for more rigid, load-bearing applications.
Ceramic Scaffolds
Though ceramics historically have been a major component of devices used in joint replacement surgeries, this material was not seriously considered as a staple of orthopedic implants until the 1990s.
Now used extensively in implants, ceramics offer a number of advantages versus metal. Besides being biologically inert, ceramics produce no wear debris and can be designed more easily to match the material properties of natural bone. The articulating surfaces on hip, knee and shoulder implants usually are composed of alumina and zirconia, two types of ceramics that are scratch-resistant and significantly harder than metal. These two ceramics also can be used on both the ball and socket components of an implant.
One of the disadvantages to using ceramics in implants is the material’s limited lifespan. With orthopedic procedures increasingly being performed on younger patients, surgeons and OEMs are eager for researchers to develop technological breakthroughs that would extend the life of ceramic implant components.
Such a breakthrough may be close. Phillips Plastics Corp., a custom injection molder of plastic, metal and ceramics based in Hudson, WI, is experimenting with bone-scaffolding technology. Designed for use in orthopedic procedures, the technology involves using porous biomaterials to help the body’s own bone to grow while also creating “pathways” for nutrients to nourish the new bone. For example, the ceramic “scaffold” that is created to foster bone growth eventually is incorporated into the patient’s natural bone, restoring it to its original condition.
“The scaffolds are made in various sizes and surgeons implant them in a patient to promote new bone growth,” said Jeff Thompson, medical market director at Phillips Plastics. “The scaffolds look like a miniature steel construction scaffold, while they can be biocompatible, ceramic, metal, or polymers. It’s a perfect structure for cell growth and at the same time offers the highest strength of any porous structures available to the marketplace.”
Once the scaffolds are ready for implantation, they either can be mixed with bone for traditional spinal fusion or can be directly inserted into defects in the vertebrae to restore the vertebrae to their original form.
A second technological breakthrough involving ceramics has been developed by Amedica Corp., an orthopedic implant firm based in Salt Lake City, UT. The company has created a silicon nitride ceramic spinal implant that is designed to restore the biomechanical integrity of the anterior, middle and posterior spine for a prolonged period.
Amedica’s spinal implant is designed to help surgically correct and stabilize the thoracolumbar spine. The FDA granted Amedica a special 510(k) marketing clearance for the ceramic spinal implant late last year.
* * *
As the demand for orthopedic implants grows, the need for devices with lifelong durability is bound to grow as well. Advances in technology and alternatives to stainless steel implants have helped increase the life of orthopedic implants in recent years, but revision surgeries to replace worn devices are still necessary. A promising new technique that uses bioceramics to promote natural bone growth may one day make revision surgeries obsolete. In the end, though, new materials that are developed must have the same characteristics as those that have been used for the last several decades. The formula, according to Boston Centerless’ Keaveney, is simple: “The material still has to be strong, it still has to be corrosive resistant, body compatible, and durable.”
SIDEBAR:
Critical Components of Total Hip and Knee Replacements
British orthopedist Sir John Charnley largely is credited with performing the first modern total hip replacement in the early 1960s. He combined a metal stem and ball with a plastic shell and used a methacrylate cement to hold the devices in place.
The stem portions of most hip implants today are composed of titanium or cobalt-chromium alloys, according to the American Academy of Orthopaedic Surgeons (AAOS). The implants are manufactured in various shapes, and some have porous surfaces to allow for bone in-growth.
The ball portion of the implant is made of cobalt-chromium alloys or ceramic materials such as aluminum oxide or zirconium oxide. The balls are polished smooth, so they can rotate easily within the prosthetic socket, AAOS research indicated. The acetabular socket can be composed of metal, ultra-high-molecular-weight polyethylene or a combination of polyethylene backed by metal.
Combined, all components of a hip implant weigh between 14 and 18 ounces, depending on the size needed. According to the AAOS, all materials used in a total hip replacement have four characteristics in common:
• Biocompatibility. They can function in the body without creating either a local or a systemic rejection response.
• Durability. They are resistant to corrosion, degradation and wear; as a result, they will retain their strength and shape for a long time. Resistance to wear is particularly significant in maintaining proper joint function and preventing further destruction of bone caused by particulate debris generated as the implant parts move against each other.
• Their mechanical properties duplicate the structures they have replaced. They must be strong enough to withstand weight-bearing loads, flexible enough to bear stress without breaking and be able to move smoothly against each other.
• They meet the highest standards. The standards extend to fabrication and quality control at a reasonable cost.
Knee implants have a similar composition to hip implants. The metal parts of knee implants are composed of titanium or cobalt-chromium alloys, and the plastic components are made of ultra-high-density polyethylene, data from the AAOS indicated. Combined, all components weigh between 15 and 20 ounces, depending on the size selected. According to the AAOS, materials used in knee implants must meet several criteria:
• Biocompatibility. They must be able to function in the body without creating a local or a systemic rejection response.
• Their mechanical properties must be able to duplicate the structures they are intended to replace. They must be strong enough to take weight-bearing loads, flexible enough to bear stress without breaking and be able to move smoothly against each other as required.
• They must retain their strength and shape for a long time. The chance of a knee replacement lasting 15 to 20 years currently is about 95%.
The number of total hip and knee implants has grown exponentially in the four decades since Charnley performed the first procedure. Generally, implants in the 1960s and 1970s were reserved for the elderly. But eventually, implants gained popularity with younger patients, helping to increase demand for the devices during the 1970s and 1980s.
In the early 1990s, the nation’s $1 billion orthopedic implant market was growing at 10% annually. The rate held steady throughout the decade and carried over into the new century, as the nation’s battle with obesity climbed to epidemic proportions and a growing number of young athletes looked to extend their sports careers (either scholastically or professionally).
The aging baby boomer generation also has added to the demand for implants, particularly those for the hip and knee. With the oldest members of this generation (an estimated 78 million people) now eligible for early retirement, industry experts predict that baby boomers will turn to the orthopedic implant market in droves to alleviate the natural wear and tear on their aging joints.
Recent research suggests this trend will continue for the next two decades. US demand for orthopedic implants is forecast to rise 9.8% annually to $23 billion in 2012, according to data from Reportlinker.com. Reconstructive joint replacements, spinal implants, orthobiologics and trauma implants are expected to provide strong growth opportunities.