Christopher Delporte, Editorial Director, Michael Barbella, Managing Editor08.04.14
The orthopedic market, while one of the largest sectors in the medical device industry, also happens to be among the most challenging. That doesn’t mean, however, that growth and opportunities for innovation are nonexistent. Companies continue to innovate and the past year has seen robust acquisition activity.
In the past year, we’ve seen a significant number of deals in orthopedics, internationally and here at home—ranging from multibillion-dollar buyouts to smaller deal-making. Stryker Corp. recently bought Small Bone Innovations for $375 million in cash. Biomet Inc. bought spine firm Lanx Inc. late last year. This spring, Biomet was the target, with its planned purchase by Zimmer Holdings Inc. for $13.4 billion (the deal has not yet closed). Wright Medical Group Inc. shed its large-joint holdings last year and is bulking up its extremities business. To that end, Wright purchased small extremities firms OrthoPro LLC and Solana Surgical LLC, for $32.5 million and $90 million, respectively. Last spring, NuVasive Inc. purchased one of its suppliers, small Ohio-based spinal implant maker ANC LLC for $4.5 million. And, Smith & Nephew plc is preparing to close on its $1.7 billion purchase of ArthroCare Corp.
Analysts and other industry-watchers predict continued orthopedic market growth, with a focus on international opportunities, minimally invasive technologies and an expanding extremities market. And, of course, as the industry adjusts to new healthcare sector demands, any system, any technology or procedure that reduces costs, increases efficiency and decreases hospital time will have an edge. The timing is right for smaller companies with transformative ideas.
This is the fifth year, as part of our Top Company Report issue, that Orthopedic Design & Technology has profiled small and midsize emerging growth firms positioning themselves alongside (perhaps with the goal of overtaking or being acquired by) larger market leaders. This year’s installment provides an overview of four orthopedic companies vying for rank, digests their technologies, examines their sectors and what’s kept them busy during the past year.
Benvenue Medical
Leadership:
• Robert Weigle, CEO
• Laurent Schaller, Founder & Chief Technical Officer
• Jeffrey Jones, Chief Operating Officer
• Victor Barajas, VP of Operations
• Barbara S. Lindsay, VP, Clinical, Regulatory and Quality Affairs
Sector: Spine/Vertebral Compression Fractures
Location: Santa Clara, Calif.
Online: www.benvenuemedical.com
Founded in 2004, private-equity-backed Benvenue Medical Inc. develops minimally invasive expandable implants for the spine. The Northern California firm, based in the south Bay Area in Santa Clara, has made its business tackling the treatment of vertebral compression fractures (VCFs).
According to the American Association of Neurological Surgeons, VCFs occur when the body in the spine collapses, which can lead to pain, deformity and loss of height. These fractures more commonly occur in the thoracic spine—the middle portion of the spine—the lower part, in particular. Osteoporosis is the most common cause of VCF, but the fractures also may be caused by trauma or tumors.
According to figures cited by Benvenue, there are 750,000 osteoporosis-related vertebral compression fractures annually in the United States, which is expected to grow as the population ages.
Surgical treatment options for VCFs include:
Benvenue also makes the Blazer-C vertebral augmentation system, which is used by physicians to create channels within the vertebral body for bone cement delivery. The Blazer-C is indicated for the treatment of pathological compression fractures of the vertebral body that may result from osteoporosis, benign lesions or malignant lesions, by creating channels in the existing spinal bone structure for the flow of polymethylmethacrylate bone cement.
The firm’s third device is the Luna interbody system, which is used in minimally invasive spinal fusion procedures for degenerative disc disease and incorporates Benvenue Medical’s proprietary implant technology. It has received the CE mark but is not currently available in the United States, though FDA review is pending.
A Good Year
So far, 2014 has been a busy year for the folks at Benvenue Medical, wracking up an FDA nod for its primary technology, securing a new round of funding, as well as the release of important study results.
On Jan. 28, the company reported receiving FDA 510(k) clearance for the Kiva VCF treatment system.
“We are excited to bring the Kiva System and its clinical benefits to the large and growing population of VCF patients in the U.S. market,” said Robert K. Weigle, CEO of Benvenue Medical. ”The VCF segment has little Level I clinical data, and we are proud to have sponsored one of the largest randomized studies in this space to date.”
The Kiva VCF is indicated for use in the reduction and treatment of spinal fractures in the thoracic and/or lumbar spine from T6-L5.
After receiving the FDA’s OK for Kiva, the company presented the results from KAST (Kiva System as a Vertebral Augmentation Treatment: A Safety and Effectiveness Trial). KAST compared Kiva to Medtronic Inc.’s balloon kyphoplasty (BKP) system. The trial results presented by Benvenue officials showed that the Kiva system ”met or exceeded” Medtronic’s system on every endpoint measured.
According to the company, the new implant approach allows the treating doctor to deliver a much more consistent result. In contrast, BKP inserts a bolus of bone cement directly into a vertebral cavity without an implant to hold it.
”The Kiva System was clinically proven in KAST, as well as in several other trials, to be better than or similar to balloon kyphoplasty, which is our most widely offered treatment,” said Sean M. Tutton, M.D., FSIR, co-principal investigator in the KAST study and professor of radiology and surgery at the Medical College of Wisconsin in Milwaukee. ”KAST sets the new standard for future trials in the VCF category. KAST results, in addition to the results of the other trials conducted, demonstrated the Kiva implant has important advantages for our patients and will serve as future guidance in clinical decision-making between VCF treatment options.”
”We are excited to provide a new alternative to the large and growing population of VCF patients in the U.S. market.” said Weigle. ”We believe the enthusiastic response we’re enjoying is a result of, among other things, the fact that government and private payers are pushing to ensure treatment effectiveness in their reimbursement decisions, and we have a growing body of peer-reviewed data that show Kiva’s clinical benefits over BKP.”
The new year also brought a new face in the front office. The company hired Jeffrey Jones as chief operating officer. Jones brings more than 20 years of related operations experience with medical technology startups and Fortune 500 companies to the newly created position for Benvenue. Jones is responsible for working with the senior management team to formulate current and long range plans, objectives and policies, as well as directing the company’s operations, manufacturing, development and quality departments. Previously, he served as vice president of operations at Acclarent, acquired by Johnson & Johnson in January 2010, where he supported sales growth and was responsible for supply chain, manufacturing operations, process engineering, materials, purchasing, facilities, and environmental health and safety. Jones also has held chief operating officer positions at a number of Bay Area medical device startups, including Polyremedy Inc., Reliant Technologies Inc., and Lumend Inc. Earlier in his career, he served as vice president of operations for Boston Scientific Corp. after it acquired EP Technologies, where he also served as vice president of operations. He holds a bachelor of science in engineering from the U.S. Military Academy at West Point and a master of business administration in management from Golden Gate University, and he is Six Sigma Black Belt certified.
June not only marked the beginning of summer, but also a new infusion of financing for the company. Benvenue completed a $64 million round of financing, with which it plans to build its U.S. commercial presence, scale up manufacturing, increase administrative functions to support overall corporate growth and provide working capital to fund growth in operating activities.
The financing is a combination of $40 million in Series E equity supplemented with $24 million in debt.The equity financing was led by new investor InterWest Partners with all existing major investors participating and Silicon Valley Bank was the sole debt provider.
”We welcome new investor InterWest Partners, and we’re gratified by the continued support from our existing investors and Silicon Valley Bank, who has been our long-standing banking partner. We believe the large investment in our company is due to Kiva’s successful U.S. launch, the Luna device bearing a CE mark and its upcoming FDA submission. We’re all very excited about the enthusiastic response we've received from the spine community,” said Weigle.
Benvenue also added Gil Kliman, M.D., from InterWest Partners to its board of directors.
The company is funded by InterWest Partners, Versant Ventures, DeNovo Ventures, Domain Associates and Technology Partners.
Independent Study Results
In October last year, an independent evaluation of the safety and effectiveness of the Kiva VCF compared with balloon kyphoplasty, found that Kiva delivered significant improvements in back pain, the firm reported. The Kiva system also resulted in significantly fewer new fractures and half the mean cement used as compared to balloon kyphoplasty. The peer-reviewed study results were published online and in the September/October edition of Pain Physician Journal, the official publication of the American Society of Interventional Pain Physicians. This was the second independent study to be published in 2013 providing positive results for the Kiva technology.
”Historically, balloon kyphoplasty has offered my osteoporotic VCF patients benefits. We evaluated Kiva as a new treatment option to see if those benefits were improved,” said Lucia Otten, M.D., of University Hospital in Bonn, Germany, and author of the study. ”Patients in our study treated with Kiva experienced a pronounced improvement in back pain over balloon kyphoplasty. Additionally, patients treated with Kiva demonstrated a lower incidence of newly occurring fractures and we used less than half the cement.”
”This study indicates that using Kiva to treat VCFs offers statistically significant advantages over balloon kyphoplasty in addressing pain, as well as in improving longer-term results by reducing future fractures,” said Robert Pflugmacher, M.D., professor of surgery at the University Hospital in Bonn.
The study, titled ”Comparison of Balloon Kyphoplasty with the New Kiva VCF System for the Treatment of Vertebral Compression Fractures,” was conducted on the basis of matched pairs, with 52 patients suffering from 68 osteoporotic fractures and followed for six months. Patients treated with balloon kyphoplasty were treated with KyphX system by Medtronic, the most common vertebral augmentation treatment in the United States. Outcome measurements used were visual analog scale (a measure of pain), Oswestry disability index (a measure of function), cement usage, cement extravasation (leakage), height restoration, and new fractures.
The study concluded several statistically significant outcomes in favor of Kiva over balloon kyphoplasty: Pain improvement was significantly better with Kiva at six months (p < 0.0001); new fractures following treatment with Kiva were significantly lower, 12 percent, than after balloon kyphoplasty, 54 percent (p < 0.0001); and mean cement used was less than half with Kiva (2.2-2.6 milliliters) vs. balloon kyphoplasty (4.7-7.5 milliliters).
Although not demonstrated in this study to be a statistically significant difference, cement extravasation was less with Kiva (23 percent) vs. balloon kyphoplasty (31 percent). Vertebral height restoration and functional improvement were equivalent in both groups.
ConforMIS
Leadership:
• Philipp Lang, M.D., Chairman, President & CEO
• Paul Weiner, Chief Financial Officer
• Daniel Steines, M.D., Chief Technology Officer
• Matthew Scott, Sr. VP, Operations
• Amita Shah, Sr. VP, Regulatory and Quality Affairs
• John Slamin, Sr. VP, Knee Implant Engineering
Sector: Knee Implants
Location: Bedford, Mass. & Burlington, Mass. (manufacturing)
Online: www.conformis.com
No two knees are exactly alike. Each of the planet’s 841 million sets of aged knee joints have subtle differences, whether it’s the size or shape of the femur and tibia (or both, in some cases), or form of the ligaments. Men, for instance, typically have larger femurs than women, while female knees usually have a greater Q angle (the angle the quadriceps and patella form with the knee joint) and are more narrow mediolaterally. There are cultural differences too: Western knees have a higher tibial torsion angle and lower varus alignment than their Japanese counterparts; East Asian males have smaller mediolateral/anteroposterior (ML/AP) ratio than Caucasian men; African-Americans have larger AP dimensions than Asians and Caucasians; and anterior cruciate ligament laxity is significantly different between Mayalsians and Westerners.
Ideally, such diversity would come with an assortment of replacements, each tailor-made to fit the patient.
For the most part, however, the selection of artificial knees in the United States is limited to a relatively small circle of standard-sized implants. There are none designed specifically for women or Far Eastern nations, nor are there any for African-Americans, Indians or Koreans.
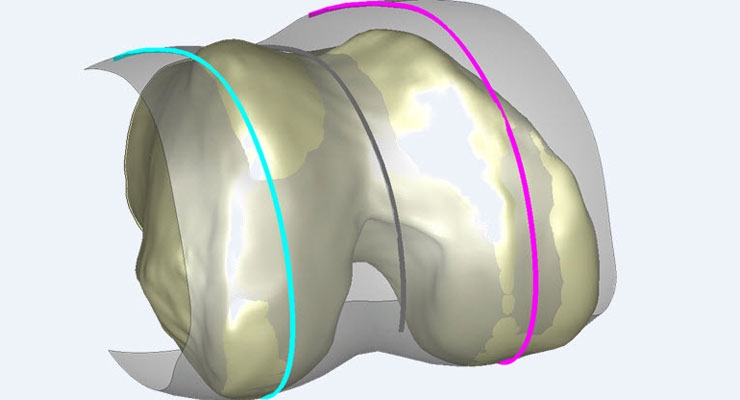
ConforMIS is hoping to change that. Founded on the simple philosophy that knee implants should fit the patient (rather than the other way around), the 10-year-old privately held company has pioneered a technology to produce custom-fit 3-D implants using patient computed tomography (CT) scans to resurface bone and minimize the amount of tissue cut out. ConforMIS is on the leading edge of a revolutionary trend in medicine in which medical devices are tailored precisely to fit the individual patient, reducing surgery times, expediting recovery, and improving patient outcomes.
”The creation of an implant that matches the anatomy perfectly is a complete change from anything that we’ve seen before. We’re actually putting in a knee replacement that is specifically designed not only from an instrument standpoint but also from the implant standpoint to that person,” said Christopher J. Cannova, M.D., an orthopedic surgeon in Bethesda, Md., who has used ConforMIS technology to custom fit implants to his patients. ”The thing that we are looking at most as we advance knee replacement, and for that matter, joint replacement surgery in general, is we ultimately want patients to forget that they have a joint replacement. The way we are able to do that is by essentially creating a stable knee that feels like their native knee. This technology and this advancement is probably the biggest thing that we’ve seen so far that allows us to do that.”
ConforMIS’ iTotal platform is touted as the only U.S. Food and Drug Administration-approved custom total knee implant system where both the artificial joint and cutting tools necessary for surgery are tailored to the individual patient. Released commercially in October 2012, the iTotal Patient-Specific Tricompartmental Knee Replacement System converts a CT knee scan to a three-dimensional model by using proprietary algorithms to map the articular surface of the joint and define the area of disease.
The software uses that information to design the customized implants and instruments, correcting the data for any underlying arthritic deformity such as bone spurs, cysts or flattening of the joint.
The company uses 3-D printing technology to produce tools called iJigs that are shaped precisely to the implant. The instruments align perfectly to a patient’s knee, but they also have placement and cutting guides that enable surgeons to make specific cuts to remove a minimal amount of bone. With these tools, inserting the implant is much like snapping a Lego piece into position exactly where it belongs, resulting in considerably less manual effort and consequently, less chance for error.
Clearly, ConforMIS implants take longer to manufacture—four weeks compared with three for an off-the-shelf implant featuring customized instruments and just one week for traditional standard-sized replacements—but the shorter recovery time and improved flexibility make it worth the wait for many patients.
”Within four months I had two total knee replacements done the ConforMIS way. I have a cousin in Colorado who had a total knee replacement done the traditional way and I was there to help her recuperate. Believe it or not, my surgery was so much easier,” Sue Birtles, 58, noted in a video testimonial on the company’s website. ”She was not able to do the things I was able to do as far as the extension and the bend. [ConforMIS] was made to fit my knee, not somebody else’s knee—not a guy’s knee, not another woman’s knee…they didn’t pull it out of a box. It was made to fit me, and to me that made more sense.”
The iTotal system is economically sensible as well: The procedure is less invasive than traditional knee replacements, so hospitals benefit from savings on inventory management, sterilization, and operating room setup and turnover. ConforMIS implants also don’t typically require blood transfusions, which can increase procedural costs by more than $2,200, according to Cleveland Clinic data. Research presented earlier this summer at the International Congress for Joint Reconstruction (ICJR) Pan Pacific Orthopaedic Congress showed that patients receiving ConforMIS implants had a blood transfusion rate of 2.4 percent—compared to 10.7 percent with standard joints.
Other data presented at ICJR found the iTotal knee replacement significantly reduced the risk of adverse events in patients undergoing total knee arthroplasty (TKA) compared with standard off-the-shelf (OTS) implants. CEO Philipp Lang said the research ”underscores the value that a customized implant provides by reducing the negative outcomes of total knee replacement without increasing, and likely decreasing, the overall cost to the healthcare system.”
The retrospective analysis included 248 TKA hospitalizations for patients who had received either the iTotal knee replacement or an OTS device between March 2010 and November 2013. The company said patients with the iTotal implant had an adverse-event rate of 1.6 percent, compared with 13.9 percent for the OTS implants. Meanwhile, an analysis of total hospital costs, excluding those associated with discharge, found no statistical difference between either group, but significantly fewer patients implanted with iTotal were discharged to acute care facilities, at 0.8 percent, compared with 7.4 percent for OTS joints.
Other studies support patient and physician testimonials on comfort and tibial fit. In a population of 63 patients treated with iTotal, 100 percent achieved alignment within ± two degrees of the neutral mechanical axis, according to data presented by Gary A. Levengood, M.D., at the British Association for Surgery of the Knee meeting in Norwich, United Kingdom, this past spring. Restoration of alignment within three degrees of neutral is a widely confirmed indicator of improved long-term survivorship in TKA.
Nashville, Tenn., orthopedic surgeon William Kurtz, M.D., presented clinical results that showed iTotal patients regaining their mean pre-operative range of motion within four months. None of the 89 patients (106 knees treated) reported any dissatisfaction in four of five Knee Scoring System categories, including pain while sitting and function while performing recreational activities. All patients receiving iTotal reported a ”normal” feeling knee seven months after the procedure, Kurtz's data found.
Also at the British Association for Surgery meeting, research demonstrated that use of iTotal significantly improves tibial fit when compared to OTS implants. ”This could play an important role in reducing knee pain and patient dissatisfaction…as well as implant loosening,” the study concluded.
Titan Spine
Leadership:
• Peter Ullrich, M.D., Co-Founder & CEO
• Kevin Gemas, Co-Founder & President
• Mark Berg, Sr. VP, Global Operations
Sector: Spinal Fusion
Location: Mequon, Wis. & Laichingen, Germany
Online: www.titanspine.com
Spinal fusion technology has been around a long time, with a widely accepted profile of safety and efficacy. Detractors, however, say that fusing vertebrae together alters the biomechanics of the spine and puts excess pressure on other vertebral levels, which can cause issues following surgery (sometimes years after), such as problems with the vertebrae above and below where the fusion took place. The anti-fusion group favors motion-preserving options such as artificial discs, dynamic stabilization technology and interspinous spacers.
Privately held startup firm Titan Spine LLC, however, is betting on the spinal fusion market.
Management of the firm, founded in 2006, claims the company was created to ”fulfill an unmet need” in the interbody fusion sector for cages designed to ”enhance fixation, preserve vertebral body integrity and help promote fusion.” Titan Spine’s technology centers around a proprietary surface treatment that creates a textured surface at the macro, micro and cellular levels—a combination the firm claims promotes new bone growth to support the fusion process.
According to estimates from London, England-based market research firm GlobalData, there’s still plenty of life left in spinal fusion. The group reports that the spinal fusion market in 2013 was valued at $4.78 billion across the 10 regions—the United States, France, Germany, Italy, Spain, the United Kingdom, Japan, Brazil, India and China. By the end of the forecast period in 2020, sales will have grown to $6.98 billion, with a compound annual growth rate (CAGR) of 5.58 percent.
GlobalData forecasts that the United States will continue to occupy the majority of the global spinal fusion market through 2020, though U.S. dominance in the market will decline from 71 percent in 2013 to 63 percent in 2020, analysts predict. It also will experience one of the lowest CAGRs over the forecast given how mature the market is in the country and newly enacted reimbursement hurdles from public health payers. Like other medical device markets, emerging economies will be a source of large growth rates. For example, China will experience double-digit growth through 2020 and this will increase its global market share from 5 percent in 2013 to 10 percent in 2020. Additionally, select established economies in the European Union will experience large growth rates over the forecast period including the United Kingdom and Italy. The primary reason for their growth, according to Global Data analysts, is the increasing procedure volumes for spinal fusion surgeries owing to favorable reimbursement levels and patients’ willingness to undergo surgery with minimally
invasive techniques. One of the major barriers affecting the spinal fusion market in the United States is the increasing public payer scrutiny of the procedure being overused. Medicare has made its
criteria for reimbursement much more stringent.
For the folks at Titan, the numbers seem to be going in the right direction. In November last year, the firm reported that it reached 18,000 implantations of its Endoskeleton interbody fusion devices since the technology’s inception and is ”rapidly approaching” a $20 million annualized sales revenue run-rate.
”These two achievements reflect the continuing rapid surgeon adoption of its proprietary interbody fusion devices and mark a paradigm shift toward devices engineered with roughened titanium surface technology,” officials wrote in a press release. There currently are more than 5,300 implants per year using the company’s technology, with more than 150 surgeon customers, officials noted in November.
Their report also noted that Titan now has more than 60 U.S. distributors, including signing a distribution agreement with Biomet Spine in Germany. The companies also reportedly are considering broadening the scope to reach physicians in additional countries within the European Union. No word yet on how Biomet’s planned $13.4 billion acquisition by Zimmer Holdings Inc. will affect the pact.
Management also reported 40 percent year-over-year revenue growth for the nine-month period ended Sept. 30, 2013. Significantly, there have been no adverse medical device reports since the company’s inception.
”One of the reasons that I believe Titan Spine’s interbody devices have resonated well with surgeons is because of the strength and design of the implant combined with the cell-signaling properties of its surface technology,” said Kade Huntsman, M.D., spine surgeon with the Salt Lake Orthopaedic Clinic in Salt Lake City, Utah, and a member of Titan’s design team. ”I like that its roughened surface technology is created from a reductive process and does not possess a coating that could have the potential for delamination or degradation. I feel very confident implanting Titan’s Endoskeleton devices.”
The Endoskeleton line of devices features Titan’s surface technology. The combination of surface levels is designed to create an optimal host-bone response and actively participate in the fusion process by promoting new bone growth, encouraging natural production of bone morphogenetic proteins (BMPs) and creating the potential for a faster and more robust fusion, company officials noted.
”We are encouraged to see several other companies that are adopting the Titan Spine approach by launching interbody devices with roughened surfaces and beginning to acknowledge shortcomings with their standard PEEK (polyetheretherketone) and smooth titanium offerings,” said Kevin Gemas, president of Titan Spine. ”We have been optimizing our surface technology and its bone formation effects… through collaboration with thought leaders in materials science and biomedical engineering and feel that our commitment to be the leaders in surface technology is the reason we are starting to see rapid acceleration in our sales growth.”
In July this year, the company received clearance from the U.S. Food and Drug Administration (FDA) for its Endoskeleton TL system, a spinal fusion system using a lateral approach. According to the company, the Endoskeleton TL represents the first lateral fusion device to feature surface technology that is designed to participate in the fusion process by creating an osteogenic response to the implant’s topography. The device uses the company’s roughened titanium surface technology, which has been shown to improve the production of osteogenic (bone growth) and angiogenic (formation of new blood vessels) factors that are critical for bone growth and fusion. The design of the TL device incorporates large windows and large internal volumes to allow for significant bone graft packing, clear CT and MRI imaging, desired bone graft loading, and the ability to pack additional bone graft material within the device following implantation, according to the company. Members of the TL design team include Kade Huntsman (quoted above); Andy Kranenburg, M.D., co-medical director of the Providence Medford Medical Center Spine Institute in Medford, Ore.; Axel Reinhardt, M.D., head of the Department of Spinal Surgery at the Specialized Orthopaedic Hospital in Potsdam, Germany; and Paul Slosar, M.D., chief medical officer for Titan Spine.
Huntsman performed the first surgeries using the Endoskeleton TL on July 9 at St. Mark’s Hospital in Salt Lake City.
Slosar noted: ”The ability to orchestrate cellular behavior and promote bone growth in response to an interbody device has not been in the lateral surgeon’s armamentarium until now. The TL is the byproduct of a unique collaboration between academic biomaterial scientists, spine surgeons, and industry experts to create a truly differentiated lateral interbody device that is designed to benefit
patients and surgeons.”
Awards & Studies
Shortly after the FDA cleared the Endoskeleton TL, the company was presented with the Whitecloud Award for Best Basic Science Research by the Scoliosis Research Society in recognition for a research paper that evaluated Titan’s surface technology. The study results demonstrate, Titan executives said, that the company’s line of Endoskeleton interbody devices promotes osteoblastic differentiation and enhanced bone-forming environment compared to devices made from PEEK.
The paper, titled ”Implant Materials Generate Different Peri-Implant Inflammatory Factors: PEEK Promotes Fibrosis and Micro-textured Titanium Promotes Osteogenic Factors,” was presented by Slosar at the International Meeting on Advanced Spine Techniques (IMAST) held July 16–19 in Valencia, Spain.
”Through this research we are better able to understand how implant surface properties influence specific inflammatory micro-environment factors,” said Barbara Boyan, Ph.D., dean of the School of Engineering at Virginia Commonwealth University and lead author of the study. ”We found that the titanium alloy surface with a complex micron scale and sub-micron scale roughness promotes a cellular response that favors bone formation. Conversely PEEK created an inflammation response that will more likely to lead to fibrous tissue formation.” According to the company, previous in-vitro research on Titan Spine’s current proprietary surface technology demonstrated a significantly enhanced osteogenic environment when compared to smooth titanium or PEEK.
In June, Belgrade, Mont.-based Bacterin International Holdings Inc. and Titan Spine received good news from a peer reviewed article that appeared in The International Journal of Spine Surgery.
Bacterin is an accredited tissue bank as well as a developer of spine products. The study, titled ”Transforaminal Lumbar Interbody Fusion Rates in Patients Using a Novel Titanium Implant and Demineralized Cancellous Allograft Bone Sponge,” reported positive results with the use of Bacterin’s OsteoSponge, a demineralized cancellous bone product for spinal fusion procedures, and Titan Spine’s Endoskeleton TT titanium cage and autograft bone.
Gerard Girasole, M.D., was the principle investigator for the journal article that evaluated OsteoSponge for interbody fusion in conjunction with Titan Spine’s Endoskeleton TT titanium cage and autograft bone. The study involved a set of patients evaluated at six months and a separate set of patients that were evaluated at one year after surgery. An independent radiologist reviewed and graded the computed tomography scans for evidence on fusion and determined the fusion rates to be 41 of 44 (93.2 percent) for the six-month group and 37 of 38 (97.4 percent) for the 12-month group. There were no radiographic device-related complications.
The impetus for the study, as stated in the abstract, was that traditional transforaminal lumbar interbody fusion (TLIF) with grafting and implant options such as iliac crest bone graft (ICBG), recombinant bone morphogenetic protein (rhBMP), and PEEK cages have been reported to achieve extremely high fusion rates. Unfortunately, these options also have been frequently cited in the literature as causing postoperative morbidity and complications at a high cost. So the researchers sought to investigate TLIF using an acid-etched, roughened titanium cage (Titan Spine’s) that upregulates osteogenesis to see if similar fusion rates to those cited for ICBG, rhBMP, and PEEK cages could be safely achieved with minimal morbidity and complications.
Expanding International Reach
Titan’s product line is commercially available in the United States and portions of Europe and recently gained market approval in Australia and New Zealand, with much of the international reach occurring recently. In June this year, the company expanded use of its Endoskeleton line of interbody devices to the United Kingdom and Spain. A week later, Titan received separate registration approval from the Australian Therapeutic Goods Administration and the New Zealand Medicines and Medical Devices Safety Authority to commercially market the Endoskeleton line.
At present, the company’s product portfolio includes the following Endoskeleton devices: TL for lumbar procedures; TAS, an anterior (from the front) lumbar interbody fusion (ALIF) device with screws; TA for ALIF procedures; TT for TLIF procedures; TO for posterior lumbar interbody fusion (performed by approaching the spine through the low back) and oblique procedures; and TC for cervical procedures.
IlluminOss Medical
Leadership:
• Dirk Kuyper, President & CEO
• Robert Rabiner, Founder & Chief Technology Officer
• Gene DiPoto, Sr. VP of Research & Development
• Beth Money, Director of Operations
Sector: Fracture Repair
Location: East Providence, R.I.
Online: www.illuminoss.com
Ultimate fighting is a tough sport: The kneebars, the joint locks, the heel hooks, and double-leg takedowns—among various other defensive moves—can cause some rather gruesome injuries. During a particularly brutal night in December 2008, Ultimate Fighting Championship lightweight Corey Hill fractured his tibia and fibula from a low kick by Dale Hartt; Razak ”The Razor” Al-Hassan dislocated his right elbow in an armbar from Steve Cantwell (he sported a large mass the size of a softball on his way backstage); and Jonathan Goulet tore his medial collateral ligament as he collapsed from a series of head punches by Mike Swick just 33 seconds into their match.
Robert Rabiner never cared much for the sport until a 2012 bout gave his fledgling company the chance to prove its worth. Rabiner is founder and chief technology officer at IlluminOss Medical Inc., an East Providence, R.I.-based firm that has developed a way to fix broken bones without screws, plates or casts (Hill would have been a prime candidate). The company’s Photodynamic Bone Stabilization System (PBSS) is not approved in the United States, but the innovation has healed several hundred patients in Europe over the last four years. Among the cured was an ultimate fighter who returned to the sport two weeks after fracturing the fifth metacarpal of his left hand.
Buoyed by its success in Europe (and recently adding Spain and Israel to the mix), IlluminOss executives currently are working with the U.S. Food and Drug Administration to launch clinical trials in America. ”It’s a much longer process getting approved here,” Rabiner told Brand RI, a monthly business publication of Rhode Island Monthly. ”We’ve spent more than $10 million on preclinical and clinical testing in support of this product and its safety. I believe this could be the next big idea.”
Venture capitalists appear to agree. Since its 2007 founding, IlluminOss has attracted $39 million in funding, with one investor calling the company’s technology ”an exceptionally versatile and powerful bone repair system.”
One of the factors contributing to the power of IlluminOss’ technology is its potential to remove the painful and costly obstacles of soft tissue damage, severe pain, temporary or permanent stiffness and long recovery times associated with traditional fracture fixation solutions (typically metal plates, screws and long incisions).
The company’s PBSS platform consists of inserting a permanent balloon filled with a cement-like substance into the bone to anchor it in place from within. The balloon not only leaves less scarring than conventional surgery for the insertion of plates and screws, but also eliminates the need for a second procedure for hardware removal after the bone heals. According to the company, the PBSS technique is ideal for both simple fractures and more serious ones, where the bone shatters into pieces and must be put back together again by surgeons. The procedure does not last very long and consists of several stages.
After first aligning the fracture manually, the surgeon makes a small incision in the skin, about three-quarters of an inch in length, and drills a small hole into the bone using a metal rod. A balloon-tipped catheter—similar to the kind used in angioplasties—then is inserted into the tiny canal inside the bone. When it reaches the fracture site, the surgeon fills the balloon with a liquid polymer that hardens with exposure to a special-frequency light. Next, a fiber-optic cable with a light on the end is fed through the same catheter; when the light is turned on, the liquid in the balloon solidifies in about 90 seconds, pushing the bone fragments back into place from within and encouraging natural healing.
One of the biggest advantages about the PBSS procedure is that patients can put weight on the broken bone within hours, and can return to their normal activities in just several weeks. The ultimate fighter who broke his metacarpal would have been out of action for at least six to eight weeks with traditional repair treatments.
”Two weeks later he went back to boxing,” Rabiner said in the Brand RI article. ”He's now using that hand—quite successfully—to once again beat up other men.”
As a startup, IlluminOss does not have an extensive list of clinical success stories. But its track record nevertheless is spotless thus far: Data presented in late 2011 at the German Congress for Orthopaedics and Trauma Surgery showed the PBSS platform is effective in treating metacarpal fractures.
In a study presented at the Congress, 12 patients were treated with IlluminOss technology between January 2010 and March 2011 for metacarpal fractures (10 with fifth metacarpal fractures and two with fourth metacarpal fractures). Eleven of the patients had a fractured ray and one sustained breaks to two metacarpal bones. The patients’ average age was 27.2 years, the median operation time was 75.8 minutes and the time interval between trauma and the procedure was 5.8 days.
Four patients received an additional locking with fine-thread screws. The participants received a two-finger splint in intrinsic-plus-position of the finger for one week after surgery, then were given a twin-tape (buddy splint) for an additional one to three weeks. The average follow-up period was 13.6 months, give or take three and one-half months. All patients had free functioning with complete extension and bending of their fingers and none had rotational error. The average DASH-Score was 31.8 points. One patient had swelling and reddening around the operation site after the procedure but it healed under conservative therapy and without secondary damage.
”IlluminOss can prove itself to be a sensible alternative treatment for metacarpal fractures,” the study concluded. ”This indication has meanwhile been extended through the development of longer balloons with greater diameter for care of fractures of long tubular bones. Herewith, an implant is available that adjusts itself to the individual medullary space of the person.”
IlluminOss also has used its technology to heal fractures in the forearm, wrist and ankle. An 81-year-old woman who fell and broke her ulna was treated with the firm’s PBSS platform and left the hospital nine hours after her fracture was aligned, stabilized and closed with three sutures. She recovered uneventfully at home and maintained her independent lifestyle, according to the company.
Similarly, an 87-year-old woman who fell and broke both wrists initially was going to be stabilized, treated with casts on both arms and sent to a nursing home for recovery. Instead, her injuries were stabilized the IlluminOss way, with the fracture aligned, the implant cured and the incision closed with two sutures within 47 minutes. The patient was in the hospital overnight and was able to move both wrists without pain the next day.
In addition, a professional saxophone musician who suffered from a metastasis in his left humerus underwent the PBSS procedure to return to work quickly. Only a week after his injury was stabilized and treated, he performed a live concert.
”Our goal is to change the way surgeons and healthcare systems think about treating older patients with fractures, change the paradigm of treatment,” CEO Dirk Kuyper said. ”The whole goal is to get them back to their normal daily routine as quickly as possible. We do that substantially faster than traditional fixation methods.”
In the past year, we’ve seen a significant number of deals in orthopedics, internationally and here at home—ranging from multibillion-dollar buyouts to smaller deal-making. Stryker Corp. recently bought Small Bone Innovations for $375 million in cash. Biomet Inc. bought spine firm Lanx Inc. late last year. This spring, Biomet was the target, with its planned purchase by Zimmer Holdings Inc. for $13.4 billion (the deal has not yet closed). Wright Medical Group Inc. shed its large-joint holdings last year and is bulking up its extremities business. To that end, Wright purchased small extremities firms OrthoPro LLC and Solana Surgical LLC, for $32.5 million and $90 million, respectively. Last spring, NuVasive Inc. purchased one of its suppliers, small Ohio-based spinal implant maker ANC LLC for $4.5 million. And, Smith & Nephew plc is preparing to close on its $1.7 billion purchase of ArthroCare Corp.
Analysts and other industry-watchers predict continued orthopedic market growth, with a focus on international opportunities, minimally invasive technologies and an expanding extremities market. And, of course, as the industry adjusts to new healthcare sector demands, any system, any technology or procedure that reduces costs, increases efficiency and decreases hospital time will have an edge. The timing is right for smaller companies with transformative ideas.
This is the fifth year, as part of our Top Company Report issue, that Orthopedic Design & Technology has profiled small and midsize emerging growth firms positioning themselves alongside (perhaps with the goal of overtaking or being acquired by) larger market leaders. This year’s installment provides an overview of four orthopedic companies vying for rank, digests their technologies, examines their sectors and what’s kept them busy during the past year.
Benvenue Medical
Leadership:
• Robert Weigle, CEO
• Laurent Schaller, Founder & Chief Technical Officer
• Jeffrey Jones, Chief Operating Officer
• Victor Barajas, VP of Operations
• Barbara S. Lindsay, VP, Clinical, Regulatory and Quality Affairs
Sector: Spine/Vertebral Compression Fractures
Location: Santa Clara, Calif.
Online: www.benvenuemedical.com
Founded in 2004, private-equity-backed Benvenue Medical Inc. develops minimally invasive expandable implants for the spine. The Northern California firm, based in the south Bay Area in Santa Clara, has made its business tackling the treatment of vertebral compression fractures (VCFs).
According to the American Association of Neurological Surgeons, VCFs occur when the body in the spine collapses, which can lead to pain, deformity and loss of height. These fractures more commonly occur in the thoracic spine—the middle portion of the spine—the lower part, in particular. Osteoporosis is the most common cause of VCF, but the fractures also may be caused by trauma or tumors.
According to figures cited by Benvenue, there are 750,000 osteoporosis-related vertebral compression fractures annually in the United States, which is expected to grow as the population ages.
Surgical treatment options for VCFs include:
- Vertebroplasty. Bone cement is injected into cracked or broken vertebrae. The cement hardens, stabilizing the fractures;
- Balloon kyphoplasty. The procedure is similar to vertebroplasty except kyphoplasty inserts a small balloon into the fracture. The balloon is inflated to create a space that is filled with bone cement to help restore vertebral height and reduce spinal deformity, according to the website Spine Universe. It also allows a thicker cement to be used, which has less risk of leaking out and causing complications, the website noted; and
- Spinal fusion, which bonds two or more vertebrae together using bone graft (naturally and artificially derived) and small spacers/cages often are used as well.
Benvenue also makes the Blazer-C vertebral augmentation system, which is used by physicians to create channels within the vertebral body for bone cement delivery. The Blazer-C is indicated for the treatment of pathological compression fractures of the vertebral body that may result from osteoporosis, benign lesions or malignant lesions, by creating channels in the existing spinal bone structure for the flow of polymethylmethacrylate bone cement.
The firm’s third device is the Luna interbody system, which is used in minimally invasive spinal fusion procedures for degenerative disc disease and incorporates Benvenue Medical’s proprietary implant technology. It has received the CE mark but is not currently available in the United States, though FDA review is pending.
A Good Year
So far, 2014 has been a busy year for the folks at Benvenue Medical, wracking up an FDA nod for its primary technology, securing a new round of funding, as well as the release of important study results.
On Jan. 28, the company reported receiving FDA 510(k) clearance for the Kiva VCF treatment system.
“We are excited to bring the Kiva System and its clinical benefits to the large and growing population of VCF patients in the U.S. market,” said Robert K. Weigle, CEO of Benvenue Medical. ”The VCF segment has little Level I clinical data, and we are proud to have sponsored one of the largest randomized studies in this space to date.”
The Kiva VCF is indicated for use in the reduction and treatment of spinal fractures in the thoracic and/or lumbar spine from T6-L5.
After receiving the FDA’s OK for Kiva, the company presented the results from KAST (Kiva System as a Vertebral Augmentation Treatment: A Safety and Effectiveness Trial). KAST compared Kiva to Medtronic Inc.’s balloon kyphoplasty (BKP) system. The trial results presented by Benvenue officials showed that the Kiva system ”met or exceeded” Medtronic’s system on every endpoint measured.
According to the company, the new implant approach allows the treating doctor to deliver a much more consistent result. In contrast, BKP inserts a bolus of bone cement directly into a vertebral cavity without an implant to hold it.
”The Kiva System was clinically proven in KAST, as well as in several other trials, to be better than or similar to balloon kyphoplasty, which is our most widely offered treatment,” said Sean M. Tutton, M.D., FSIR, co-principal investigator in the KAST study and professor of radiology and surgery at the Medical College of Wisconsin in Milwaukee. ”KAST sets the new standard for future trials in the VCF category. KAST results, in addition to the results of the other trials conducted, demonstrated the Kiva implant has important advantages for our patients and will serve as future guidance in clinical decision-making between VCF treatment options.”
”We are excited to provide a new alternative to the large and growing population of VCF patients in the U.S. market.” said Weigle. ”We believe the enthusiastic response we’re enjoying is a result of, among other things, the fact that government and private payers are pushing to ensure treatment effectiveness in their reimbursement decisions, and we have a growing body of peer-reviewed data that show Kiva’s clinical benefits over BKP.”
The new year also brought a new face in the front office. The company hired Jeffrey Jones as chief operating officer. Jones brings more than 20 years of related operations experience with medical technology startups and Fortune 500 companies to the newly created position for Benvenue. Jones is responsible for working with the senior management team to formulate current and long range plans, objectives and policies, as well as directing the company’s operations, manufacturing, development and quality departments. Previously, he served as vice president of operations at Acclarent, acquired by Johnson & Johnson in January 2010, where he supported sales growth and was responsible for supply chain, manufacturing operations, process engineering, materials, purchasing, facilities, and environmental health and safety. Jones also has held chief operating officer positions at a number of Bay Area medical device startups, including Polyremedy Inc., Reliant Technologies Inc., and Lumend Inc. Earlier in his career, he served as vice president of operations for Boston Scientific Corp. after it acquired EP Technologies, where he also served as vice president of operations. He holds a bachelor of science in engineering from the U.S. Military Academy at West Point and a master of business administration in management from Golden Gate University, and he is Six Sigma Black Belt certified.
June not only marked the beginning of summer, but also a new infusion of financing for the company. Benvenue completed a $64 million round of financing, with which it plans to build its U.S. commercial presence, scale up manufacturing, increase administrative functions to support overall corporate growth and provide working capital to fund growth in operating activities.
The financing is a combination of $40 million in Series E equity supplemented with $24 million in debt.The equity financing was led by new investor InterWest Partners with all existing major investors participating and Silicon Valley Bank was the sole debt provider.
”We welcome new investor InterWest Partners, and we’re gratified by the continued support from our existing investors and Silicon Valley Bank, who has been our long-standing banking partner. We believe the large investment in our company is due to Kiva’s successful U.S. launch, the Luna device bearing a CE mark and its upcoming FDA submission. We’re all very excited about the enthusiastic response we've received from the spine community,” said Weigle.
Benvenue also added Gil Kliman, M.D., from InterWest Partners to its board of directors.
The company is funded by InterWest Partners, Versant Ventures, DeNovo Ventures, Domain Associates and Technology Partners.
Independent Study Results
In October last year, an independent evaluation of the safety and effectiveness of the Kiva VCF compared with balloon kyphoplasty, found that Kiva delivered significant improvements in back pain, the firm reported. The Kiva system also resulted in significantly fewer new fractures and half the mean cement used as compared to balloon kyphoplasty. The peer-reviewed study results were published online and in the September/October edition of Pain Physician Journal, the official publication of the American Society of Interventional Pain Physicians. This was the second independent study to be published in 2013 providing positive results for the Kiva technology.
”Historically, balloon kyphoplasty has offered my osteoporotic VCF patients benefits. We evaluated Kiva as a new treatment option to see if those benefits were improved,” said Lucia Otten, M.D., of University Hospital in Bonn, Germany, and author of the study. ”Patients in our study treated with Kiva experienced a pronounced improvement in back pain over balloon kyphoplasty. Additionally, patients treated with Kiva demonstrated a lower incidence of newly occurring fractures and we used less than half the cement.”
”This study indicates that using Kiva to treat VCFs offers statistically significant advantages over balloon kyphoplasty in addressing pain, as well as in improving longer-term results by reducing future fractures,” said Robert Pflugmacher, M.D., professor of surgery at the University Hospital in Bonn.
The study, titled ”Comparison of Balloon Kyphoplasty with the New Kiva VCF System for the Treatment of Vertebral Compression Fractures,” was conducted on the basis of matched pairs, with 52 patients suffering from 68 osteoporotic fractures and followed for six months. Patients treated with balloon kyphoplasty were treated with KyphX system by Medtronic, the most common vertebral augmentation treatment in the United States. Outcome measurements used were visual analog scale (a measure of pain), Oswestry disability index (a measure of function), cement usage, cement extravasation (leakage), height restoration, and new fractures.
The study concluded several statistically significant outcomes in favor of Kiva over balloon kyphoplasty: Pain improvement was significantly better with Kiva at six months (p < 0.0001); new fractures following treatment with Kiva were significantly lower, 12 percent, than after balloon kyphoplasty, 54 percent (p < 0.0001); and mean cement used was less than half with Kiva (2.2-2.6 milliliters) vs. balloon kyphoplasty (4.7-7.5 milliliters).
Although not demonstrated in this study to be a statistically significant difference, cement extravasation was less with Kiva (23 percent) vs. balloon kyphoplasty (31 percent). Vertebral height restoration and functional improvement were equivalent in both groups.
ConforMIS
Leadership:
• Philipp Lang, M.D., Chairman, President & CEO
• Paul Weiner, Chief Financial Officer
• Daniel Steines, M.D., Chief Technology Officer
• Matthew Scott, Sr. VP, Operations
• Amita Shah, Sr. VP, Regulatory and Quality Affairs
• John Slamin, Sr. VP, Knee Implant Engineering
Sector: Knee Implants
Location: Bedford, Mass. & Burlington, Mass. (manufacturing)
Online: www.conformis.com
No two knees are exactly alike. Each of the planet’s 841 million sets of aged knee joints have subtle differences, whether it’s the size or shape of the femur and tibia (or both, in some cases), or form of the ligaments. Men, for instance, typically have larger femurs than women, while female knees usually have a greater Q angle (the angle the quadriceps and patella form with the knee joint) and are more narrow mediolaterally. There are cultural differences too: Western knees have a higher tibial torsion angle and lower varus alignment than their Japanese counterparts; East Asian males have smaller mediolateral/anteroposterior (ML/AP) ratio than Caucasian men; African-Americans have larger AP dimensions than Asians and Caucasians; and anterior cruciate ligament laxity is significantly different between Mayalsians and Westerners.
Ideally, such diversity would come with an assortment of replacements, each tailor-made to fit the patient.
For the most part, however, the selection of artificial knees in the United States is limited to a relatively small circle of standard-sized implants. There are none designed specifically for women or Far Eastern nations, nor are there any for African-Americans, Indians or Koreans.
ConforMIS is hoping to change that. Founded on the simple philosophy that knee implants should fit the patient (rather than the other way around), the 10-year-old privately held company has pioneered a technology to produce custom-fit 3-D implants using patient computed tomography (CT) scans to resurface bone and minimize the amount of tissue cut out. ConforMIS is on the leading edge of a revolutionary trend in medicine in which medical devices are tailored precisely to fit the individual patient, reducing surgery times, expediting recovery, and improving patient outcomes.
”The creation of an implant that matches the anatomy perfectly is a complete change from anything that we’ve seen before. We’re actually putting in a knee replacement that is specifically designed not only from an instrument standpoint but also from the implant standpoint to that person,” said Christopher J. Cannova, M.D., an orthopedic surgeon in Bethesda, Md., who has used ConforMIS technology to custom fit implants to his patients. ”The thing that we are looking at most as we advance knee replacement, and for that matter, joint replacement surgery in general, is we ultimately want patients to forget that they have a joint replacement. The way we are able to do that is by essentially creating a stable knee that feels like their native knee. This technology and this advancement is probably the biggest thing that we’ve seen so far that allows us to do that.”
ConforMIS’ iTotal platform is touted as the only U.S. Food and Drug Administration-approved custom total knee implant system where both the artificial joint and cutting tools necessary for surgery are tailored to the individual patient. Released commercially in October 2012, the iTotal Patient-Specific Tricompartmental Knee Replacement System converts a CT knee scan to a three-dimensional model by using proprietary algorithms to map the articular surface of the joint and define the area of disease.
The software uses that information to design the customized implants and instruments, correcting the data for any underlying arthritic deformity such as bone spurs, cysts or flattening of the joint.
The company uses 3-D printing technology to produce tools called iJigs that are shaped precisely to the implant. The instruments align perfectly to a patient’s knee, but they also have placement and cutting guides that enable surgeons to make specific cuts to remove a minimal amount of bone. With these tools, inserting the implant is much like snapping a Lego piece into position exactly where it belongs, resulting in considerably less manual effort and consequently, less chance for error.
Clearly, ConforMIS implants take longer to manufacture—four weeks compared with three for an off-the-shelf implant featuring customized instruments and just one week for traditional standard-sized replacements—but the shorter recovery time and improved flexibility make it worth the wait for many patients.
”Within four months I had two total knee replacements done the ConforMIS way. I have a cousin in Colorado who had a total knee replacement done the traditional way and I was there to help her recuperate. Believe it or not, my surgery was so much easier,” Sue Birtles, 58, noted in a video testimonial on the company’s website. ”She was not able to do the things I was able to do as far as the extension and the bend. [ConforMIS] was made to fit my knee, not somebody else’s knee—not a guy’s knee, not another woman’s knee…they didn’t pull it out of a box. It was made to fit me, and to me that made more sense.”
The iTotal system is economically sensible as well: The procedure is less invasive than traditional knee replacements, so hospitals benefit from savings on inventory management, sterilization, and operating room setup and turnover. ConforMIS implants also don’t typically require blood transfusions, which can increase procedural costs by more than $2,200, according to Cleveland Clinic data. Research presented earlier this summer at the International Congress for Joint Reconstruction (ICJR) Pan Pacific Orthopaedic Congress showed that patients receiving ConforMIS implants had a blood transfusion rate of 2.4 percent—compared to 10.7 percent with standard joints.
Other data presented at ICJR found the iTotal knee replacement significantly reduced the risk of adverse events in patients undergoing total knee arthroplasty (TKA) compared with standard off-the-shelf (OTS) implants. CEO Philipp Lang said the research ”underscores the value that a customized implant provides by reducing the negative outcomes of total knee replacement without increasing, and likely decreasing, the overall cost to the healthcare system.”
The retrospective analysis included 248 TKA hospitalizations for patients who had received either the iTotal knee replacement or an OTS device between March 2010 and November 2013. The company said patients with the iTotal implant had an adverse-event rate of 1.6 percent, compared with 13.9 percent for the OTS implants. Meanwhile, an analysis of total hospital costs, excluding those associated with discharge, found no statistical difference between either group, but significantly fewer patients implanted with iTotal were discharged to acute care facilities, at 0.8 percent, compared with 7.4 percent for OTS joints.
Other studies support patient and physician testimonials on comfort and tibial fit. In a population of 63 patients treated with iTotal, 100 percent achieved alignment within ± two degrees of the neutral mechanical axis, according to data presented by Gary A. Levengood, M.D., at the British Association for Surgery of the Knee meeting in Norwich, United Kingdom, this past spring. Restoration of alignment within three degrees of neutral is a widely confirmed indicator of improved long-term survivorship in TKA.
Nashville, Tenn., orthopedic surgeon William Kurtz, M.D., presented clinical results that showed iTotal patients regaining their mean pre-operative range of motion within four months. None of the 89 patients (106 knees treated) reported any dissatisfaction in four of five Knee Scoring System categories, including pain while sitting and function while performing recreational activities. All patients receiving iTotal reported a ”normal” feeling knee seven months after the procedure, Kurtz's data found.
Also at the British Association for Surgery meeting, research demonstrated that use of iTotal significantly improves tibial fit when compared to OTS implants. ”This could play an important role in reducing knee pain and patient dissatisfaction…as well as implant loosening,” the study concluded.
Titan Spine
Leadership:
• Peter Ullrich, M.D., Co-Founder & CEO
• Kevin Gemas, Co-Founder & President
• Mark Berg, Sr. VP, Global Operations
Sector: Spinal Fusion
Location: Mequon, Wis. & Laichingen, Germany
Online: www.titanspine.com
Spinal fusion technology has been around a long time, with a widely accepted profile of safety and efficacy. Detractors, however, say that fusing vertebrae together alters the biomechanics of the spine and puts excess pressure on other vertebral levels, which can cause issues following surgery (sometimes years after), such as problems with the vertebrae above and below where the fusion took place. The anti-fusion group favors motion-preserving options such as artificial discs, dynamic stabilization technology and interspinous spacers.
Privately held startup firm Titan Spine LLC, however, is betting on the spinal fusion market.
Management of the firm, founded in 2006, claims the company was created to ”fulfill an unmet need” in the interbody fusion sector for cages designed to ”enhance fixation, preserve vertebral body integrity and help promote fusion.” Titan Spine’s technology centers around a proprietary surface treatment that creates a textured surface at the macro, micro and cellular levels—a combination the firm claims promotes new bone growth to support the fusion process.
According to estimates from London, England-based market research firm GlobalData, there’s still plenty of life left in spinal fusion. The group reports that the spinal fusion market in 2013 was valued at $4.78 billion across the 10 regions—the United States, France, Germany, Italy, Spain, the United Kingdom, Japan, Brazil, India and China. By the end of the forecast period in 2020, sales will have grown to $6.98 billion, with a compound annual growth rate (CAGR) of 5.58 percent.
GlobalData forecasts that the United States will continue to occupy the majority of the global spinal fusion market through 2020, though U.S. dominance in the market will decline from 71 percent in 2013 to 63 percent in 2020, analysts predict. It also will experience one of the lowest CAGRs over the forecast given how mature the market is in the country and newly enacted reimbursement hurdles from public health payers. Like other medical device markets, emerging economies will be a source of large growth rates. For example, China will experience double-digit growth through 2020 and this will increase its global market share from 5 percent in 2013 to 10 percent in 2020. Additionally, select established economies in the European Union will experience large growth rates over the forecast period including the United Kingdom and Italy. The primary reason for their growth, according to Global Data analysts, is the increasing procedure volumes for spinal fusion surgeries owing to favorable reimbursement levels and patients’ willingness to undergo surgery with minimally
invasive techniques. One of the major barriers affecting the spinal fusion market in the United States is the increasing public payer scrutiny of the procedure being overused. Medicare has made its
criteria for reimbursement much more stringent.
For the folks at Titan, the numbers seem to be going in the right direction. In November last year, the firm reported that it reached 18,000 implantations of its Endoskeleton interbody fusion devices since the technology’s inception and is ”rapidly approaching” a $20 million annualized sales revenue run-rate.
”These two achievements reflect the continuing rapid surgeon adoption of its proprietary interbody fusion devices and mark a paradigm shift toward devices engineered with roughened titanium surface technology,” officials wrote in a press release. There currently are more than 5,300 implants per year using the company’s technology, with more than 150 surgeon customers, officials noted in November.
Their report also noted that Titan now has more than 60 U.S. distributors, including signing a distribution agreement with Biomet Spine in Germany. The companies also reportedly are considering broadening the scope to reach physicians in additional countries within the European Union. No word yet on how Biomet’s planned $13.4 billion acquisition by Zimmer Holdings Inc. will affect the pact.
Management also reported 40 percent year-over-year revenue growth for the nine-month period ended Sept. 30, 2013. Significantly, there have been no adverse medical device reports since the company’s inception.
”One of the reasons that I believe Titan Spine’s interbody devices have resonated well with surgeons is because of the strength and design of the implant combined with the cell-signaling properties of its surface technology,” said Kade Huntsman, M.D., spine surgeon with the Salt Lake Orthopaedic Clinic in Salt Lake City, Utah, and a member of Titan’s design team. ”I like that its roughened surface technology is created from a reductive process and does not possess a coating that could have the potential for delamination or degradation. I feel very confident implanting Titan’s Endoskeleton devices.”
The Endoskeleton line of devices features Titan’s surface technology. The combination of surface levels is designed to create an optimal host-bone response and actively participate in the fusion process by promoting new bone growth, encouraging natural production of bone morphogenetic proteins (BMPs) and creating the potential for a faster and more robust fusion, company officials noted.
”We are encouraged to see several other companies that are adopting the Titan Spine approach by launching interbody devices with roughened surfaces and beginning to acknowledge shortcomings with their standard PEEK (polyetheretherketone) and smooth titanium offerings,” said Kevin Gemas, president of Titan Spine. ”We have been optimizing our surface technology and its bone formation effects… through collaboration with thought leaders in materials science and biomedical engineering and feel that our commitment to be the leaders in surface technology is the reason we are starting to see rapid acceleration in our sales growth.”
In July this year, the company received clearance from the U.S. Food and Drug Administration (FDA) for its Endoskeleton TL system, a spinal fusion system using a lateral approach. According to the company, the Endoskeleton TL represents the first lateral fusion device to feature surface technology that is designed to participate in the fusion process by creating an osteogenic response to the implant’s topography. The device uses the company’s roughened titanium surface technology, which has been shown to improve the production of osteogenic (bone growth) and angiogenic (formation of new blood vessels) factors that are critical for bone growth and fusion. The design of the TL device incorporates large windows and large internal volumes to allow for significant bone graft packing, clear CT and MRI imaging, desired bone graft loading, and the ability to pack additional bone graft material within the device following implantation, according to the company. Members of the TL design team include Kade Huntsman (quoted above); Andy Kranenburg, M.D., co-medical director of the Providence Medford Medical Center Spine Institute in Medford, Ore.; Axel Reinhardt, M.D., head of the Department of Spinal Surgery at the Specialized Orthopaedic Hospital in Potsdam, Germany; and Paul Slosar, M.D., chief medical officer for Titan Spine.
Huntsman performed the first surgeries using the Endoskeleton TL on July 9 at St. Mark’s Hospital in Salt Lake City.
Slosar noted: ”The ability to orchestrate cellular behavior and promote bone growth in response to an interbody device has not been in the lateral surgeon’s armamentarium until now. The TL is the byproduct of a unique collaboration between academic biomaterial scientists, spine surgeons, and industry experts to create a truly differentiated lateral interbody device that is designed to benefit
patients and surgeons.”
Awards & Studies
Shortly after the FDA cleared the Endoskeleton TL, the company was presented with the Whitecloud Award for Best Basic Science Research by the Scoliosis Research Society in recognition for a research paper that evaluated Titan’s surface technology. The study results demonstrate, Titan executives said, that the company’s line of Endoskeleton interbody devices promotes osteoblastic differentiation and enhanced bone-forming environment compared to devices made from PEEK.
The paper, titled ”Implant Materials Generate Different Peri-Implant Inflammatory Factors: PEEK Promotes Fibrosis and Micro-textured Titanium Promotes Osteogenic Factors,” was presented by Slosar at the International Meeting on Advanced Spine Techniques (IMAST) held July 16–19 in Valencia, Spain.
”Through this research we are better able to understand how implant surface properties influence specific inflammatory micro-environment factors,” said Barbara Boyan, Ph.D., dean of the School of Engineering at Virginia Commonwealth University and lead author of the study. ”We found that the titanium alloy surface with a complex micron scale and sub-micron scale roughness promotes a cellular response that favors bone formation. Conversely PEEK created an inflammation response that will more likely to lead to fibrous tissue formation.” According to the company, previous in-vitro research on Titan Spine’s current proprietary surface technology demonstrated a significantly enhanced osteogenic environment when compared to smooth titanium or PEEK.
In June, Belgrade, Mont.-based Bacterin International Holdings Inc. and Titan Spine received good news from a peer reviewed article that appeared in The International Journal of Spine Surgery.
Bacterin is an accredited tissue bank as well as a developer of spine products. The study, titled ”Transforaminal Lumbar Interbody Fusion Rates in Patients Using a Novel Titanium Implant and Demineralized Cancellous Allograft Bone Sponge,” reported positive results with the use of Bacterin’s OsteoSponge, a demineralized cancellous bone product for spinal fusion procedures, and Titan Spine’s Endoskeleton TT titanium cage and autograft bone.
Gerard Girasole, M.D., was the principle investigator for the journal article that evaluated OsteoSponge for interbody fusion in conjunction with Titan Spine’s Endoskeleton TT titanium cage and autograft bone. The study involved a set of patients evaluated at six months and a separate set of patients that were evaluated at one year after surgery. An independent radiologist reviewed and graded the computed tomography scans for evidence on fusion and determined the fusion rates to be 41 of 44 (93.2 percent) for the six-month group and 37 of 38 (97.4 percent) for the 12-month group. There were no radiographic device-related complications.
The impetus for the study, as stated in the abstract, was that traditional transforaminal lumbar interbody fusion (TLIF) with grafting and implant options such as iliac crest bone graft (ICBG), recombinant bone morphogenetic protein (rhBMP), and PEEK cages have been reported to achieve extremely high fusion rates. Unfortunately, these options also have been frequently cited in the literature as causing postoperative morbidity and complications at a high cost. So the researchers sought to investigate TLIF using an acid-etched, roughened titanium cage (Titan Spine’s) that upregulates osteogenesis to see if similar fusion rates to those cited for ICBG, rhBMP, and PEEK cages could be safely achieved with minimal morbidity and complications.
Expanding International Reach
Titan’s product line is commercially available in the United States and portions of Europe and recently gained market approval in Australia and New Zealand, with much of the international reach occurring recently. In June this year, the company expanded use of its Endoskeleton line of interbody devices to the United Kingdom and Spain. A week later, Titan received separate registration approval from the Australian Therapeutic Goods Administration and the New Zealand Medicines and Medical Devices Safety Authority to commercially market the Endoskeleton line.
At present, the company’s product portfolio includes the following Endoskeleton devices: TL for lumbar procedures; TAS, an anterior (from the front) lumbar interbody fusion (ALIF) device with screws; TA for ALIF procedures; TT for TLIF procedures; TO for posterior lumbar interbody fusion (performed by approaching the spine through the low back) and oblique procedures; and TC for cervical procedures.
IlluminOss Medical
Leadership:
• Dirk Kuyper, President & CEO
• Robert Rabiner, Founder & Chief Technology Officer
• Gene DiPoto, Sr. VP of Research & Development
• Beth Money, Director of Operations
Sector: Fracture Repair
Location: East Providence, R.I.
Online: www.illuminoss.com
Ultimate fighting is a tough sport: The kneebars, the joint locks, the heel hooks, and double-leg takedowns—among various other defensive moves—can cause some rather gruesome injuries. During a particularly brutal night in December 2008, Ultimate Fighting Championship lightweight Corey Hill fractured his tibia and fibula from a low kick by Dale Hartt; Razak ”The Razor” Al-Hassan dislocated his right elbow in an armbar from Steve Cantwell (he sported a large mass the size of a softball on his way backstage); and Jonathan Goulet tore his medial collateral ligament as he collapsed from a series of head punches by Mike Swick just 33 seconds into their match.
Robert Rabiner never cared much for the sport until a 2012 bout gave his fledgling company the chance to prove its worth. Rabiner is founder and chief technology officer at IlluminOss Medical Inc., an East Providence, R.I.-based firm that has developed a way to fix broken bones without screws, plates or casts (Hill would have been a prime candidate). The company’s Photodynamic Bone Stabilization System (PBSS) is not approved in the United States, but the innovation has healed several hundred patients in Europe over the last four years. Among the cured was an ultimate fighter who returned to the sport two weeks after fracturing the fifth metacarpal of his left hand.
Buoyed by its success in Europe (and recently adding Spain and Israel to the mix), IlluminOss executives currently are working with the U.S. Food and Drug Administration to launch clinical trials in America. ”It’s a much longer process getting approved here,” Rabiner told Brand RI, a monthly business publication of Rhode Island Monthly. ”We’ve spent more than $10 million on preclinical and clinical testing in support of this product and its safety. I believe this could be the next big idea.”
Venture capitalists appear to agree. Since its 2007 founding, IlluminOss has attracted $39 million in funding, with one investor calling the company’s technology ”an exceptionally versatile and powerful bone repair system.”
One of the factors contributing to the power of IlluminOss’ technology is its potential to remove the painful and costly obstacles of soft tissue damage, severe pain, temporary or permanent stiffness and long recovery times associated with traditional fracture fixation solutions (typically metal plates, screws and long incisions).
The company’s PBSS platform consists of inserting a permanent balloon filled with a cement-like substance into the bone to anchor it in place from within. The balloon not only leaves less scarring than conventional surgery for the insertion of plates and screws, but also eliminates the need for a second procedure for hardware removal after the bone heals. According to the company, the PBSS technique is ideal for both simple fractures and more serious ones, where the bone shatters into pieces and must be put back together again by surgeons. The procedure does not last very long and consists of several stages.
After first aligning the fracture manually, the surgeon makes a small incision in the skin, about three-quarters of an inch in length, and drills a small hole into the bone using a metal rod. A balloon-tipped catheter—similar to the kind used in angioplasties—then is inserted into the tiny canal inside the bone. When it reaches the fracture site, the surgeon fills the balloon with a liquid polymer that hardens with exposure to a special-frequency light. Next, a fiber-optic cable with a light on the end is fed through the same catheter; when the light is turned on, the liquid in the balloon solidifies in about 90 seconds, pushing the bone fragments back into place from within and encouraging natural healing.
One of the biggest advantages about the PBSS procedure is that patients can put weight on the broken bone within hours, and can return to their normal activities in just several weeks. The ultimate fighter who broke his metacarpal would have been out of action for at least six to eight weeks with traditional repair treatments.
”Two weeks later he went back to boxing,” Rabiner said in the Brand RI article. ”He's now using that hand—quite successfully—to once again beat up other men.”
As a startup, IlluminOss does not have an extensive list of clinical success stories. But its track record nevertheless is spotless thus far: Data presented in late 2011 at the German Congress for Orthopaedics and Trauma Surgery showed the PBSS platform is effective in treating metacarpal fractures.
In a study presented at the Congress, 12 patients were treated with IlluminOss technology between January 2010 and March 2011 for metacarpal fractures (10 with fifth metacarpal fractures and two with fourth metacarpal fractures). Eleven of the patients had a fractured ray and one sustained breaks to two metacarpal bones. The patients’ average age was 27.2 years, the median operation time was 75.8 minutes and the time interval between trauma and the procedure was 5.8 days.
Four patients received an additional locking with fine-thread screws. The participants received a two-finger splint in intrinsic-plus-position of the finger for one week after surgery, then were given a twin-tape (buddy splint) for an additional one to three weeks. The average follow-up period was 13.6 months, give or take three and one-half months. All patients had free functioning with complete extension and bending of their fingers and none had rotational error. The average DASH-Score was 31.8 points. One patient had swelling and reddening around the operation site after the procedure but it healed under conservative therapy and without secondary damage.
”IlluminOss can prove itself to be a sensible alternative treatment for metacarpal fractures,” the study concluded. ”This indication has meanwhile been extended through the development of longer balloons with greater diameter for care of fractures of long tubular bones. Herewith, an implant is available that adjusts itself to the individual medullary space of the person.”
IlluminOss also has used its technology to heal fractures in the forearm, wrist and ankle. An 81-year-old woman who fell and broke her ulna was treated with the firm’s PBSS platform and left the hospital nine hours after her fracture was aligned, stabilized and closed with three sutures. She recovered uneventfully at home and maintained her independent lifestyle, according to the company.
Similarly, an 87-year-old woman who fell and broke both wrists initially was going to be stabilized, treated with casts on both arms and sent to a nursing home for recovery. Instead, her injuries were stabilized the IlluminOss way, with the fracture aligned, the implant cured and the incision closed with two sutures within 47 minutes. The patient was in the hospital overnight and was able to move both wrists without pain the next day.
In addition, a professional saxophone musician who suffered from a metastasis in his left humerus underwent the PBSS procedure to return to work quickly. Only a week after his injury was stabilized and treated, he performed a live concert.
”Our goal is to change the way surgeons and healthcare systems think about treating older patients with fractures, change the paradigm of treatment,” CEO Dirk Kuyper said. ”The whole goal is to get them back to their normal daily routine as quickly as possible. We do that substantially faster than traditional fixation methods.”