
Michael Barbella, Managing Editor03.22.17
Rick E. Parsons, M.D., isn’t a big fan of hospitals.
His aversion is quite paradoxical, however, considering he’s a self-professed “adventure junkie” and orthopedic surgeon who’s worked at four different hospitals in North Carolina and Tennessee during his 28-year career. Parsons is also an avid cycler, skier, and mountain climber prone to the kinds of injuries he fixes, and has entrusted his health to other surgeons on occasion.
So what’s his beef with hospitals?
Time and resource management, for starters. Having worked in hospitals for most of his career, Parsons has experienced more than his fair share of scheduling snafus and O.R. delays resulting from inadequate facilities oversight and/or emergency room demands. He also takes exception to the growing patient load at U.S. healthcare institutions, which can affect both surgical timing and physician performance. Studies show that only 38 percent of surgeries performed in a hospital setting are completed within their scheduled timeframe, and double booking runs rampant.
Such demanding workloads are part of the reason Parsons prefers mending damaged shoulders and knees in an outpatient setting. Specifically, he favors working in ambulatory surgery centers (ASCs)—facilities that provide same-day surgical care, including diagnostic and preventive procedures. More than 5,400 Medicare-certified ASCs currently exist in the United States, according to Medicare Payment Advisory Commission 2015 data; common services provided at ASCs include cataract surgery, upper GI endoscopy, colonoscopy, and spinal injections (lumbar, sacral).
Since its inception in 1970, physicians have led the development of ASCs. By working in an outpatient rather than a hospital setting, doctors gain more direct control of their surgical practices. They can also schedule procedures more conveniently, assemble teams of specially-trained and highly skilled staff, ensure the equipment and supplies being used are best suited to their technique(s), and design facilities tailored to their medical specialties.
 “As an orthopedic surgeon, several of the procedures I conduct can be performed in the outpatient setting,” Parsons told the Alexandria, Va.-based Ambulatory Surgery Center Association’s (ASCA) Campaign for Advancing Surgical Care. “In an ASC, I don’t face the same scheduling hurdles which can plague hospitals, and...patient load flows smoother. ASCs provide a high-touch environment. From pre-op to discharge, patients often receive one-on-one care.”
“As an orthopedic surgeon, several of the procedures I conduct can be performed in the outpatient setting,” Parsons told the Alexandria, Va.-based Ambulatory Surgery Center Association’s (ASCA) Campaign for Advancing Surgical Care. “In an ASC, I don’t face the same scheduling hurdles which can plague hospitals, and...patient load flows smoother. ASCs provide a high-touch environment. From pre-op to discharge, patients often receive one-on-one care.”
And that care is less costly, too. An ASCA study determined that ASCs reduce U.S. healthcare costs by more than $38 billion annually, as the prices charged at these centers are significantly lower than hospital outpatient department prices in all markets. The report also estimated an annual savings of $55 billion depending on the percentage of procedures that migrate to ASCs and the mix of patient preference for these centers as opposed to hospital outpatient settings.
The cost savings in bone and joint procedures is particularly significant: Researchers at the Children’s Hospital of Philadelphia (Pa.) found a 17 to 43 percent price reduction depending on the orthopedic procedure, when the surgery was performed at an ASC rather than a university-based institution. Clinicians attributed the savings to more efficient use of time and resources due to streamlined care processes conducted at ambulatory surgery centers.
The study’s authors examined the direct costs of 1,021 surgical bone and joint procedures in which patients chose to undergo their procedures in a hospital or an ASC setting. The study defined direct costs as goods and services such as drugs, implants, laboratory, and radiology services.
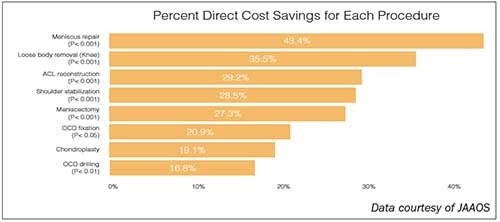
Of eight procedures studied, meniscus repair offered the most considerable savings in an ASC, reducing costs by 43.4 percent, according to data published in the Journal of the American Academy of Orthopaedic Surgeons (JAAOS). Loose body removal (knee) is 35.5 percent cheaper in the outpatient setting, followed by anterior cruciate ligament reconstruction (a 29.2 percent savings), shoulder stabilization (a 28.5 percent cost reduction), meniscectomy (a 27.3 percent savings), osteochondritis dissecans (OCD) fixation (a 20.9 percent lower), chondroplasty (a 19.1 percent savings), and OCD drilling (a 16.8 percent savings).
“If orthopedic practices gained access to an ASC for day surgery, they would be able to deliver the same care at a decreased cost and improve patient satisfaction by offering the convenience of care location options,” lead study author Peter D. Fabricant, M.D., M.P.H., of the Hospital for Special Surgery (New York, N.Y.), noted to JAAOS. “From the patient and family perspective, care closer to one’s home and family is of higher value.”
And, justifiably, priceless.
His aversion is quite paradoxical, however, considering he’s a self-professed “adventure junkie” and orthopedic surgeon who’s worked at four different hospitals in North Carolina and Tennessee during his 28-year career. Parsons is also an avid cycler, skier, and mountain climber prone to the kinds of injuries he fixes, and has entrusted his health to other surgeons on occasion.
So what’s his beef with hospitals?
Time and resource management, for starters. Having worked in hospitals for most of his career, Parsons has experienced more than his fair share of scheduling snafus and O.R. delays resulting from inadequate facilities oversight and/or emergency room demands. He also takes exception to the growing patient load at U.S. healthcare institutions, which can affect both surgical timing and physician performance. Studies show that only 38 percent of surgeries performed in a hospital setting are completed within their scheduled timeframe, and double booking runs rampant.
Such demanding workloads are part of the reason Parsons prefers mending damaged shoulders and knees in an outpatient setting. Specifically, he favors working in ambulatory surgery centers (ASCs)—facilities that provide same-day surgical care, including diagnostic and preventive procedures. More than 5,400 Medicare-certified ASCs currently exist in the United States, according to Medicare Payment Advisory Commission 2015 data; common services provided at ASCs include cataract surgery, upper GI endoscopy, colonoscopy, and spinal injections (lumbar, sacral).
Since its inception in 1970, physicians have led the development of ASCs. By working in an outpatient rather than a hospital setting, doctors gain more direct control of their surgical practices. They can also schedule procedures more conveniently, assemble teams of specially-trained and highly skilled staff, ensure the equipment and supplies being used are best suited to their technique(s), and design facilities tailored to their medical specialties.
And that care is less costly, too. An ASCA study determined that ASCs reduce U.S. healthcare costs by more than $38 billion annually, as the prices charged at these centers are significantly lower than hospital outpatient department prices in all markets. The report also estimated an annual savings of $55 billion depending on the percentage of procedures that migrate to ASCs and the mix of patient preference for these centers as opposed to hospital outpatient settings.
The cost savings in bone and joint procedures is particularly significant: Researchers at the Children’s Hospital of Philadelphia (Pa.) found a 17 to 43 percent price reduction depending on the orthopedic procedure, when the surgery was performed at an ASC rather than a university-based institution. Clinicians attributed the savings to more efficient use of time and resources due to streamlined care processes conducted at ambulatory surgery centers.
The study’s authors examined the direct costs of 1,021 surgical bone and joint procedures in which patients chose to undergo their procedures in a hospital or an ASC setting. The study defined direct costs as goods and services such as drugs, implants, laboratory, and radiology services.
Of eight procedures studied, meniscus repair offered the most considerable savings in an ASC, reducing costs by 43.4 percent, according to data published in the Journal of the American Academy of Orthopaedic Surgeons (JAAOS). Loose body removal (knee) is 35.5 percent cheaper in the outpatient setting, followed by anterior cruciate ligament reconstruction (a 29.2 percent savings), shoulder stabilization (a 28.5 percent cost reduction), meniscectomy (a 27.3 percent savings), osteochondritis dissecans (OCD) fixation (a 20.9 percent lower), chondroplasty (a 19.1 percent savings), and OCD drilling (a 16.8 percent savings).
“If orthopedic practices gained access to an ASC for day surgery, they would be able to deliver the same care at a decreased cost and improve patient satisfaction by offering the convenience of care location options,” lead study author Peter D. Fabricant, M.D., M.P.H., of the Hospital for Special Surgery (New York, N.Y.), noted to JAAOS. “From the patient and family perspective, care closer to one’s home and family is of higher value.”
And, justifiably, priceless.















