Sam Brusco, Associate Editor05.29.18
After years of teaching spin classes, 41-year-old Kirkland, Wash., fitness instructor Rhianna Ryer found herself in the unfortunate and severely uncomfortable position of developing bone-on-bone arthritis in her knee. The debilitating, degenerative joint condition rendered her unable to push herself and her students in her classes. For years she took injections to manage the symptoms, but the temporary fix was not a proper fit for her highly active lifestyle.
“Nothing was helping, and actually my girlfriend who is a physical therapist had told me about the Conformis [knee replacement],” Ryer recounted in a patient testimonial video. “She said ‘you need to look into this—it’s designed for younger, active adults.’”
An improvement on “off-the-shelf” knee implants, Conformis’ iTotal is a custom-made, patient-specific total knee replacement engineered to mimic the natural knee—including both its unique shape and the manner in which it flexes and extends. The tailored fit results in optimal bone preservation, meaning less of the patient’s anatomy is removed during surgery. The result is often an expedited recovery time, allowing patients to get back on their feet to resume their fitness regimen in relatively short order.
“After the surgery, I could teach dance classes, and I could also do squats, and I could do yoga poses—which I couldn’t before because I lacked the flexibility,” Ryer said. “Now I teach 12 classes a week. I teach six spinning classes, I teach three Pilates classes, and I teach three boot camp classes.”
Conformis manufactures custom metal knee implants using image-to-implant technology. Production begins with a CT scan of the hip, affected knee, and ankle so the leg is realigned to the neutral mechanical axis. A series of Conformis algorithms—dubbed iFit technology—converts the 2D scan of the knee into a 3D model that maps the joint’s articular surface and distinctly defines the affected area. Each customized femoral and tibial implant is then designed by the software, including customized “iJig” instrumentation used for just the one implantation.
The manufacturing process employed to produce customized implants associated with complex surgical procedures like total knee arthroplasty, while ultimately beneficial for patients, is a challenging endeavor. Conformis must be able to produce each knee implant rapidly to prevent delays in scheduling surgery. As more surgeons adopt usage of customized knee implants, the process must also be scalable to match the increase in demand. Both of these must be feasible without any negative effects on the implant’s quality or precision, as well.
To safely speed the process, Conformis uses additive manufacturing technology to print a wax mold used as a form for the metal femoral component of the knee. The iJig single-use instrumentation is also manufactured via 3D printing, with each set pre-navigated for the specific implant and fully sterilized. Each implant is manufactured using the cobalt-chromium-molybdenum alloy specified in the ASTM F75 industry standard. Conformis then packages the implant and ships it along with the iJig instruments to the healthcare facility.
A customized manufacturing model allows new implant designs to be incorporated into production immediately, so innovations like new material applications and technologies can reach clinicians and patients more quickly. Conformis’ successful application of this model (the company has unveiled a new product iteration every year since 2008) capitalizes on two significant, and in this case, symbiotic trends affecting the orthopedic implant manufacturing market—the increased adoption of patient-specific designs as well as the use of additive manufacturing. In order to comprehensively examine these factors, among others, affecting the implant manufacturing market, Orthopedic Design & Technology spoke with four orthopedic manufacturing professionals over the past few weeks:
Brandon Beckendorf, director of engineering at Orchid Design, a division of Orchid Orthopedic Solutions, a Lansing, Mich.-based provider of orthopedic medical device outsourcing, offering contract design and manufacturing services.
Michael Carter, vice president and general manager of Stryker Corporation’s Allendale, N.J.-based Spine Division, which designs, manufactures, and services a full range of spinal products for both traditional and minimally invasive surgical procedures.
Tony DeHart, director of sales and marketing at Micro Machine Company, a Kalamazoo, Mich.-based precision contract manufacturer of medical products primarily to the orthopedic and spinal industries.
John MacDonald, president of AIP Precision Machining, a Daytona Beach, Fla.-based provider of precision machining services for the medical industry.
Sam Brusco: Which sector of the orthopedic implant market is experiencing the most growth, and why?
Brandon Beckendorf: From our eyes at Orchid Design, there is significant new product development activity in the extremities sector, particularly in the foot and ankle markets.
Tony DeHart: Current trends show that one of the fastest growing markets in the implant industry continues to be the spinal fusion and fixation devices segment. The aging baby boomer population, along with increased insurance availability, are factors in the compounded annual growth we are seeing with this segment.
John MacDonald: For the past 35 years, AIP has specialized in machining plastic and composite materials only, no metallic materials. Therefore, our exposure to the implant market is limited to such materials. We have seen steady growth in the PEEK spinal implant market with materials such as Solvay’s Zeniva and Invibio’s Optima.
Brusco: What trends are most significantly affecting the state of the orthopedic implant manufacturing market?
Beckendorf: Three trends that we are seeing are more outsourcing, supplier consolidation, and additive manufacturing. OEMs want to focus on marketing and distribution while trusting more of their product development and manufacturing to suppliers that are becoming stronger and more capable. Contract suppliers are also consolidating so that they can be responsive to the growth, quality, cost, and delivery requirements of their customers. Additive implant manufacturing is a growing technology that is driving change as well.
Michael Carter: Advances in additive manufacturing continue to impact the spinal implants market in important ways. One example is Stryker’s Tritanium Technology, which allows for the production of randomized yet reproducible porous structures1 that would be difficult or impossible to create using traditional manufacturing techniques. The Tritanium material features interconnected architecture with rugged irregular pore sizes and shapes designed to mimic cancellous bone.1 These new 3D-printed implants join a variety of other implant types, providing spine surgeons with a range of options to address their preferences and meet the needs of their patients.
DeHart: Adoption of new minimally invasive procedures, as well as better refinement in the spinal surgical robots and navigation systems is adding to the growth potential in this manufacturing market. An increasing number of surgeons have adopted these techniques to improve repeatability and accuracy, thereby improving patient outcomes.
MacDonald: Price and delivery. OEMs seem to be trending more and more toward a “just in time” methodology. We have responded by adding resources to meet these ever-changing demands. Additionally, we have moved toward more automation in order to increase capacity as well as partner with the OEM to create win-win ordering cycles, which serve both AIP and the OEM.
Brusco: How are innovative manufacturing techniques expanding the possibilities of implant designs? Or how are conventional manufacturing methods being updated/tuned for innovative implant designs?
Beckendorf: Additive manufacturing allows for new designs that were impossible with conventional machining techniques, which can be seen with the many interbody cages now on the market that were manufactured using additive methods.
Carter: Additive manufacturing continues to change the landscape of orthopedic implant creation. In contrast to traditional manufacturing methods such as injection molding, machining, forming, or joining, additive manufacturing is a process that creates three-dimensional objects by adding layer upon layer of material. Additive manufacturing allows Stryker to push beyond the constraints of conventional manufacturing to create new implant designs that are “inspired by bone.”
Stryker’s high-resolution additive manufacturing process allows the company the ability to consistently produce randomized yet reproducible1 porous structures. Each implant is generated from a single master computer model, providing the ability to create a metal porous matrix for a given model and size of a particular product virtually identical to that which was originally tested and validated. The process enables Tritanium cages to be designed and built with pinpoint precision, optimizing pore size, porosity, geometry, and surface texture to help achieve fusion.
While additive manufacturing may appear to be a recent development in the creation of spinal implants, Stryker began collaborations with top doctoral programs at leading universities in the United Kingdom and Ireland in 2001 to industrialize 3D printing for the healthcare industry. Tritanium is the culmination of more than 15 years of extensive research, development, and validation in material science and manufacturing, and it has been utilized clinically in hip and knee applications for more than 10 years—with more than 300,000 orthopedic devices implanted. In fact, the manufacturing of Tritanium technology is now in its third generation, and today Stryker makes and sells more orthopedic implants using additive manufacturing than any company in the world.
DeHart: Implant design has been greatly influenced by the increased presence of additive manufacturing in the market. This process has allowed greater freedom during design to maximize both internal and external features while helping to promote bone growth.
Brusco: What are some best practices to successfully employ design for manufacturability (DFM) for orthopedic implant manufacture?
Beckendorf: By definition, DFM is a methodology to change a design in order to reduce the cost of making parts while retaining product function. Thus, DFM should begin with establishing cost and performance goals for the implant. From there, many concepts can be refined using a concept selection matrix that incorporates manufacturing cost estimates. Working with a supplier with diverse manufacturing methods up front can make a big impact on the quality of the analysis and the ultimate outcome of achieving cost reduction. Ultimately, the more feedback that can be incorporated from manufacturing into the design concepts prior to locking into a design, the better the outcome will be. I am proud to work at a company where this is the norm.
Carter: We are focused on transforming bright ideas into exciting new products made with Tritanium In-Growth Technology.10 A key part of this effort is ensuring that we are meeting the needs of our surgeon customers and their patients—one of the most important considerations in the design and manufacture of orthopedic implants.
In the development of Tritanium implants, Stryker consulted a team of surgeons and received valuable feedback that helped guide decision-making. In addition, Stryker specifically engineered Tritanium’s porous matrix based on studies that examined which geometry and pore size would provide a favorable environment for cells to attach and multiply within the structure of the spine.1,7,11
Enabled by AMagine, Stryker’s proprietary approach to implant creation using additive manufacturing, Tritanium is inspired by the microstructure of cancellous bone1 and deliberately designed for fusion. Its unique porous structure is designed to create a favorable environment for cell attachment and proliferation, as demonstrated in an in-vitro study,1,12* and may be able to wick or retain fluid when compared to traditional titanium material.3
Another key to advancing the field of orthopedic implants is continued research and scientific evaluation. Stryker’s Spine division is committed to supporting research and pre-clinical studies on Tritanium In-Growth Technology.10
MacDonald: Involve your contract manufacturing partner as soon as possible, listen to each other, and do not let logical design change proposals get bogged down in regulatory and internal bottlenecks. Some of the solutions offered up by CMs provide such great benefits, but at times are shelved due to the lack of willingness to work through the paperwork and the lack of personnel labor to bring about the proposal.
Brusco: Which new or existing materials are customers requesting to be used for orthopedic implant manufacture?
Beckendorf: We see many requests for the established materials such as Ti-6Al-4V, 316L, cobalt chromium, UHMWPE, PEEK, and zirconium. Coating technologies are also emerging that have the potential to impact osseointegration and prevent infection.
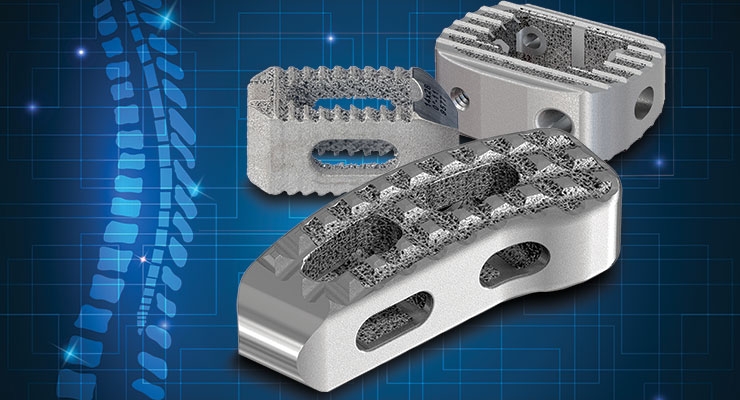
Carter: Traditionally, cages used in lumbar interbody fusion procedures have been made of allograft bone (donated bone from a bone bank) or materials such as carbon fiber, PEEK (polyetheretherketone polymer), or titanium. However, surgeons now have the option of using devices made from a novel, highly porous titanium alloy for spinal fusion procedures—Tritanium. Tritanium Technology allows for the creation of porous structures designed to mimic cancellous bone in pore size, level of porosity, and interconnectivity of the pores.1 This “precise randomization”1 of fully interconnected pores differs from other technologies featuring longitudinal channels and traverse windows that create a uniform lattice structure, as well as cages offering porosity that is only present on the surface.
Tritanium cages are engineered for stability,2 designed to minimize subsidence,3,4 and created to allow imaging.5 The roughened porous surfaces are designed to enhance interconnectivity and provide a stronger interface with surrounding bone compared to a smooth surface.6-9 Tritanium cages are intelligently designed to closely fit the anatomy of the disc space and are offered in a variety of widths, lengths, heights, and lordotic angles to accommodate a variety of patient anatomies. The cages are being well-received by surgeon users and continue to gain momentum. Since their launch, the Spine division has sold nearly 26,000 Tritanium Posterior Lumbar (PL) and Tritanium Anterior Cervical (C) Cages, combined.
Based on this success, new implants are being developed—a reflection of Stryker’s commitment to Tritanium technology as an important contribution to the future of spinal implants. Stryker previewed another new Tritanium implant, the Tritanium TL Posterior Lumbar Cage, at the American Association of Neurological Surgeons 2018 meeting in April. The Tritanium TL Cage complements the Tritanium PL Cage, and together they offer alternative posterior lumbar solutions for spine surgeons and their patients.
DeHart: Titanium and Titanium alloys still represent the largest share of the orthopedic implant market. With its widely known properties of bio-compatibility, high strength-to-weight ratio, and corrosion resistance it continues to be the most requested material type.
Brusco: How much (or little) are you seeing additive manufacturing being used to make the final orthopedic implant product?
Beckendorf: We have all seen how the utilization of additive manufacturing in the spine market for interbody cages has greatly increased over the last several years. This is an excellent application for additive manufacturing, given the porosity and surface texture desired for device performance. Additionally, in joint reconstruction, additive bone ingrowth surfaces are being integrated into the implants for non-cemented applications.
DeHart: With many well-known OEMs leading the way in product development, there has been an increase in implants produced utilizing additive manufacturing brought into the market place. This technology is being used in not only production applications, but in patient- specific procedures.
Brusco: What trends and challenges do you expect to impact the orthopedic implant manufacturing market over the next five years?
Beckendorf: Regulatory requirements associated with cleaning, biocompatibility, sterilization, process validations, and risk management demand higher competencies from implant manufacturers than ever before. Thus, I think we will see a continued consolidation and reduction of suppliers due to the regulatory requirements that implant manufacturers must satisfy. Additionally, I think that the industry has only scratched the surface on how additive manufacturing can help companies differentiate their product offering and improve patient outcomes.
MacDonald: Skilled and experienced manufacturing, quality, and procurement professional shortages will continue to strain the manufacturing industry at all levels. We need to support trade schools and apprentice programs in order to make manufacturing “sexy” again. There are some incredibly rewarding and exciting careers in this field, yet such a shortage of talent to fill these positions. Our type of machining is more a mix of art and science, which cannot be learned without a desire to create something different each week and the satisfaction gained from such work. Those two traits are the starting point for such a career, the third is the willingness to invest the extensive time to learn such a craft.
References
“Nothing was helping, and actually my girlfriend who is a physical therapist had told me about the Conformis [knee replacement],” Ryer recounted in a patient testimonial video. “She said ‘you need to look into this—it’s designed for younger, active adults.’”
An improvement on “off-the-shelf” knee implants, Conformis’ iTotal is a custom-made, patient-specific total knee replacement engineered to mimic the natural knee—including both its unique shape and the manner in which it flexes and extends. The tailored fit results in optimal bone preservation, meaning less of the patient’s anatomy is removed during surgery. The result is often an expedited recovery time, allowing patients to get back on their feet to resume their fitness regimen in relatively short order.
“After the surgery, I could teach dance classes, and I could also do squats, and I could do yoga poses—which I couldn’t before because I lacked the flexibility,” Ryer said. “Now I teach 12 classes a week. I teach six spinning classes, I teach three Pilates classes, and I teach three boot camp classes.”
Conformis manufactures custom metal knee implants using image-to-implant technology. Production begins with a CT scan of the hip, affected knee, and ankle so the leg is realigned to the neutral mechanical axis. A series of Conformis algorithms—dubbed iFit technology—converts the 2D scan of the knee into a 3D model that maps the joint’s articular surface and distinctly defines the affected area. Each customized femoral and tibial implant is then designed by the software, including customized “iJig” instrumentation used for just the one implantation.
The manufacturing process employed to produce customized implants associated with complex surgical procedures like total knee arthroplasty, while ultimately beneficial for patients, is a challenging endeavor. Conformis must be able to produce each knee implant rapidly to prevent delays in scheduling surgery. As more surgeons adopt usage of customized knee implants, the process must also be scalable to match the increase in demand. Both of these must be feasible without any negative effects on the implant’s quality or precision, as well.
To safely speed the process, Conformis uses additive manufacturing technology to print a wax mold used as a form for the metal femoral component of the knee. The iJig single-use instrumentation is also manufactured via 3D printing, with each set pre-navigated for the specific implant and fully sterilized. Each implant is manufactured using the cobalt-chromium-molybdenum alloy specified in the ASTM F75 industry standard. Conformis then packages the implant and ships it along with the iJig instruments to the healthcare facility.
A customized manufacturing model allows new implant designs to be incorporated into production immediately, so innovations like new material applications and technologies can reach clinicians and patients more quickly. Conformis’ successful application of this model (the company has unveiled a new product iteration every year since 2008) capitalizes on two significant, and in this case, symbiotic trends affecting the orthopedic implant manufacturing market—the increased adoption of patient-specific designs as well as the use of additive manufacturing. In order to comprehensively examine these factors, among others, affecting the implant manufacturing market, Orthopedic Design & Technology spoke with four orthopedic manufacturing professionals over the past few weeks:
Brandon Beckendorf, director of engineering at Orchid Design, a division of Orchid Orthopedic Solutions, a Lansing, Mich.-based provider of orthopedic medical device outsourcing, offering contract design and manufacturing services.
Michael Carter, vice president and general manager of Stryker Corporation’s Allendale, N.J.-based Spine Division, which designs, manufactures, and services a full range of spinal products for both traditional and minimally invasive surgical procedures.
Tony DeHart, director of sales and marketing at Micro Machine Company, a Kalamazoo, Mich.-based precision contract manufacturer of medical products primarily to the orthopedic and spinal industries.
John MacDonald, president of AIP Precision Machining, a Daytona Beach, Fla.-based provider of precision machining services for the medical industry.
Sam Brusco: Which sector of the orthopedic implant market is experiencing the most growth, and why?
Brandon Beckendorf: From our eyes at Orchid Design, there is significant new product development activity in the extremities sector, particularly in the foot and ankle markets.
Tony DeHart: Current trends show that one of the fastest growing markets in the implant industry continues to be the spinal fusion and fixation devices segment. The aging baby boomer population, along with increased insurance availability, are factors in the compounded annual growth we are seeing with this segment.
John MacDonald: For the past 35 years, AIP has specialized in machining plastic and composite materials only, no metallic materials. Therefore, our exposure to the implant market is limited to such materials. We have seen steady growth in the PEEK spinal implant market with materials such as Solvay’s Zeniva and Invibio’s Optima.
Brusco: What trends are most significantly affecting the state of the orthopedic implant manufacturing market?
Beckendorf: Three trends that we are seeing are more outsourcing, supplier consolidation, and additive manufacturing. OEMs want to focus on marketing and distribution while trusting more of their product development and manufacturing to suppliers that are becoming stronger and more capable. Contract suppliers are also consolidating so that they can be responsive to the growth, quality, cost, and delivery requirements of their customers. Additive implant manufacturing is a growing technology that is driving change as well.
Michael Carter: Advances in additive manufacturing continue to impact the spinal implants market in important ways. One example is Stryker’s Tritanium Technology, which allows for the production of randomized yet reproducible porous structures1 that would be difficult or impossible to create using traditional manufacturing techniques. The Tritanium material features interconnected architecture with rugged irregular pore sizes and shapes designed to mimic cancellous bone.1 These new 3D-printed implants join a variety of other implant types, providing spine surgeons with a range of options to address their preferences and meet the needs of their patients.
DeHart: Adoption of new minimally invasive procedures, as well as better refinement in the spinal surgical robots and navigation systems is adding to the growth potential in this manufacturing market. An increasing number of surgeons have adopted these techniques to improve repeatability and accuracy, thereby improving patient outcomes.
MacDonald: Price and delivery. OEMs seem to be trending more and more toward a “just in time” methodology. We have responded by adding resources to meet these ever-changing demands. Additionally, we have moved toward more automation in order to increase capacity as well as partner with the OEM to create win-win ordering cycles, which serve both AIP and the OEM.
Brusco: How are innovative manufacturing techniques expanding the possibilities of implant designs? Or how are conventional manufacturing methods being updated/tuned for innovative implant designs?
Beckendorf: Additive manufacturing allows for new designs that were impossible with conventional machining techniques, which can be seen with the many interbody cages now on the market that were manufactured using additive methods.
Carter: Additive manufacturing continues to change the landscape of orthopedic implant creation. In contrast to traditional manufacturing methods such as injection molding, machining, forming, or joining, additive manufacturing is a process that creates three-dimensional objects by adding layer upon layer of material. Additive manufacturing allows Stryker to push beyond the constraints of conventional manufacturing to create new implant designs that are “inspired by bone.”
Stryker’s high-resolution additive manufacturing process allows the company the ability to consistently produce randomized yet reproducible1 porous structures. Each implant is generated from a single master computer model, providing the ability to create a metal porous matrix for a given model and size of a particular product virtually identical to that which was originally tested and validated. The process enables Tritanium cages to be designed and built with pinpoint precision, optimizing pore size, porosity, geometry, and surface texture to help achieve fusion.
While additive manufacturing may appear to be a recent development in the creation of spinal implants, Stryker began collaborations with top doctoral programs at leading universities in the United Kingdom and Ireland in 2001 to industrialize 3D printing for the healthcare industry. Tritanium is the culmination of more than 15 years of extensive research, development, and validation in material science and manufacturing, and it has been utilized clinically in hip and knee applications for more than 10 years—with more than 300,000 orthopedic devices implanted. In fact, the manufacturing of Tritanium technology is now in its third generation, and today Stryker makes and sells more orthopedic implants using additive manufacturing than any company in the world.
DeHart: Implant design has been greatly influenced by the increased presence of additive manufacturing in the market. This process has allowed greater freedom during design to maximize both internal and external features while helping to promote bone growth.
Brusco: What are some best practices to successfully employ design for manufacturability (DFM) for orthopedic implant manufacture?
Beckendorf: By definition, DFM is a methodology to change a design in order to reduce the cost of making parts while retaining product function. Thus, DFM should begin with establishing cost and performance goals for the implant. From there, many concepts can be refined using a concept selection matrix that incorporates manufacturing cost estimates. Working with a supplier with diverse manufacturing methods up front can make a big impact on the quality of the analysis and the ultimate outcome of achieving cost reduction. Ultimately, the more feedback that can be incorporated from manufacturing into the design concepts prior to locking into a design, the better the outcome will be. I am proud to work at a company where this is the norm.
Carter: We are focused on transforming bright ideas into exciting new products made with Tritanium In-Growth Technology.10 A key part of this effort is ensuring that we are meeting the needs of our surgeon customers and their patients—one of the most important considerations in the design and manufacture of orthopedic implants.
In the development of Tritanium implants, Stryker consulted a team of surgeons and received valuable feedback that helped guide decision-making. In addition, Stryker specifically engineered Tritanium’s porous matrix based on studies that examined which geometry and pore size would provide a favorable environment for cells to attach and multiply within the structure of the spine.1,7,11
Enabled by AMagine, Stryker’s proprietary approach to implant creation using additive manufacturing, Tritanium is inspired by the microstructure of cancellous bone1 and deliberately designed for fusion. Its unique porous structure is designed to create a favorable environment for cell attachment and proliferation, as demonstrated in an in-vitro study,1,12* and may be able to wick or retain fluid when compared to traditional titanium material.3
Another key to advancing the field of orthopedic implants is continued research and scientific evaluation. Stryker’s Spine division is committed to supporting research and pre-clinical studies on Tritanium In-Growth Technology.10
- A pre-clinical animal study was conducted to compare the biomechanical, radiographic, and histological performance of spinal implants with different surface technologies in an ovine lumbar interbody fusion model. The interbody fusion cages involved in this study included traditional PEEK cages, plasma-sprayed titanium-coated PEEK cages, and Stryker’s 3D-printed, highly porous Tritanium PL cages. The study abstract was titled “Biomechanical and Histologic Comparison of a Novel 3D-Printed Porous Titanium Interbody Cage to PEEK.”13 (No correlation to human clinical outcomes has been demonstrated or established.)
- A recent wicking experiment demonstrated that a cube built with Tritanium material was able to wick fluid into the porous structure under specified conditions,6 and also absorb and hold fluid inside the porous structure.6 This laboratory experiment was performed using heparinized porcine bone marrow aspirate. (No correlation to human clinical outcomes has been demonstrated or established.)
- A cell proliferation experiment in which a coupon built with Tritanium material demonstrated that osteoblasts (cells) infiltrated, attached to, and proliferated on the porosity of the Tritanium technology.14 This laboratory experiment was performed with heparinized porcine bone marrow aspirate. (No correlation to human clinical outcomes has been demonstrated or established.)
MacDonald: Involve your contract manufacturing partner as soon as possible, listen to each other, and do not let logical design change proposals get bogged down in regulatory and internal bottlenecks. Some of the solutions offered up by CMs provide such great benefits, but at times are shelved due to the lack of willingness to work through the paperwork and the lack of personnel labor to bring about the proposal.
Brusco: Which new or existing materials are customers requesting to be used for orthopedic implant manufacture?
Beckendorf: We see many requests for the established materials such as Ti-6Al-4V, 316L, cobalt chromium, UHMWPE, PEEK, and zirconium. Coating technologies are also emerging that have the potential to impact osseointegration and prevent infection.
Carter: Traditionally, cages used in lumbar interbody fusion procedures have been made of allograft bone (donated bone from a bone bank) or materials such as carbon fiber, PEEK (polyetheretherketone polymer), or titanium. However, surgeons now have the option of using devices made from a novel, highly porous titanium alloy for spinal fusion procedures—Tritanium. Tritanium Technology allows for the creation of porous structures designed to mimic cancellous bone in pore size, level of porosity, and interconnectivity of the pores.1 This “precise randomization”1 of fully interconnected pores differs from other technologies featuring longitudinal channels and traverse windows that create a uniform lattice structure, as well as cages offering porosity that is only present on the surface.
Tritanium cages are engineered for stability,2 designed to minimize subsidence,3,4 and created to allow imaging.5 The roughened porous surfaces are designed to enhance interconnectivity and provide a stronger interface with surrounding bone compared to a smooth surface.6-9 Tritanium cages are intelligently designed to closely fit the anatomy of the disc space and are offered in a variety of widths, lengths, heights, and lordotic angles to accommodate a variety of patient anatomies. The cages are being well-received by surgeon users and continue to gain momentum. Since their launch, the Spine division has sold nearly 26,000 Tritanium Posterior Lumbar (PL) and Tritanium Anterior Cervical (C) Cages, combined.
Based on this success, new implants are being developed—a reflection of Stryker’s commitment to Tritanium technology as an important contribution to the future of spinal implants. Stryker previewed another new Tritanium implant, the Tritanium TL Posterior Lumbar Cage, at the American Association of Neurological Surgeons 2018 meeting in April. The Tritanium TL Cage complements the Tritanium PL Cage, and together they offer alternative posterior lumbar solutions for spine surgeons and their patients.
DeHart: Titanium and Titanium alloys still represent the largest share of the orthopedic implant market. With its widely known properties of bio-compatibility, high strength-to-weight ratio, and corrosion resistance it continues to be the most requested material type.
Brusco: How much (or little) are you seeing additive manufacturing being used to make the final orthopedic implant product?
Beckendorf: We have all seen how the utilization of additive manufacturing in the spine market for interbody cages has greatly increased over the last several years. This is an excellent application for additive manufacturing, given the porosity and surface texture desired for device performance. Additionally, in joint reconstruction, additive bone ingrowth surfaces are being integrated into the implants for non-cemented applications.
DeHart: With many well-known OEMs leading the way in product development, there has been an increase in implants produced utilizing additive manufacturing brought into the market place. This technology is being used in not only production applications, but in patient- specific procedures.
Brusco: What trends and challenges do you expect to impact the orthopedic implant manufacturing market over the next five years?
Beckendorf: Regulatory requirements associated with cleaning, biocompatibility, sterilization, process validations, and risk management demand higher competencies from implant manufacturers than ever before. Thus, I think we will see a continued consolidation and reduction of suppliers due to the regulatory requirements that implant manufacturers must satisfy. Additionally, I think that the industry has only scratched the surface on how additive manufacturing can help companies differentiate their product offering and improve patient outcomes.
MacDonald: Skilled and experienced manufacturing, quality, and procurement professional shortages will continue to strain the manufacturing industry at all levels. We need to support trade schools and apprentice programs in order to make manufacturing “sexy” again. There are some incredibly rewarding and exciting careers in this field, yet such a shortage of talent to fill these positions. Our type of machining is more a mix of art and science, which cannot be learned without a desire to create something different each week and the satisfaction gained from such work. Those two traits are the starting point for such a career, the third is the willingness to invest the extensive time to learn such a craft.
References
- Karageorgiou V, Kaplan D. (2005) Porosity of 3D biomaterial scaffolds and osteogenesis. Biomaterials, 26, 5474-5491.
- PROJ44960 | Coefficient of friction memo.
- PROJ0000054457 | Tritanium C subsidence marketing memo.
- PROJ42624 | Subsidence memo.
- PROJ0000054459 | Tritanium C implant imaging marketing memo.
- RD0000050927: Tritanium material capillary evaluation.
- Webster TJ, Ejiofor JU. (2004) Increased osteoblast adhesion on nanophase metals; Ti, Ti6AI4V, and CoCrMo. Biomaterials. 25, 4731-4739.
- Oldani C and Dominguez A (2012). Titanium as a Biomaterial for Implants. Recent Advances in Arthroplasty. Dr. Samo Fokter (Ed.). ISBN: 978-953-307-990-5. InTech.
- Deligianni DD, Katsala N, Ladas S et al. Effect of surface roughness of the titanium alloy Ti-6Al-4V on human bone marrow cell response and on protein adsorption. Biomaterials. 2001;22(11):1241-51.
- PROJ43909 | Tritanium technology claim support memo.
- Bobyn JD, Pilliar RM, Cameron HU, Weatherly GC. (1980) The optimum pore size for the fixation of porous-surfaced metal implants by the ingrowth of bone. Clinical Orthopaedics and Related Research, 150, 263-270.
- RD0000053710: Tritanium cell infiltration and attachment experiment. *No correlation to human clinical outcomes has been demonstrated or established
- McGilvray, Kirk C. et al. Biomechanical and Histologic Comparison of a Novel 3-D Printed Porous Titanium Interbody Cage to PEEK, Spine J. 2016; Volume 16, Issue 10, S363-S364.
- Olivares-Navarrete R, Gittens RA, Schneider JM, et al. Osteoblasts exhibit a more differentiated phenotype and increased bone morphogenetic protein production on titanium alloy substrates than on poly-ether-ether-ketone. Spine J. 2012;12(3):265–72.