Maria Shepherd, President and Founder, Medi-Vantage11.18.20
Obesity causes multiple health issues, and the COVID-19 pandemic is only adding to the problem, causing the worldwide epidemic of obesity to endure and proliferate. According to the CDC, the prevalence of obesity increased between 1999–2000 through 2017–2018, from 30.5 percent to 42.4 percent, respectively, and the prevalence of morbid obesity increased from 4.7 percent to 9.2 percent.1 These increases are climbing fast (Table 1). In a previous ODT column, I reported greater than 39 percent of adults were obese in 2016 (up from 35.7 percent of adults in 2009/10).2 The co-morbidities associated with obesity are daunting and include cardiovascular disease, type 2 diabetes, cancer,3 and musculoskeletal disorders.4 Each of these co-morbidities predisposes COVID-19 patients to require hospitalization, often including ICU admissions.
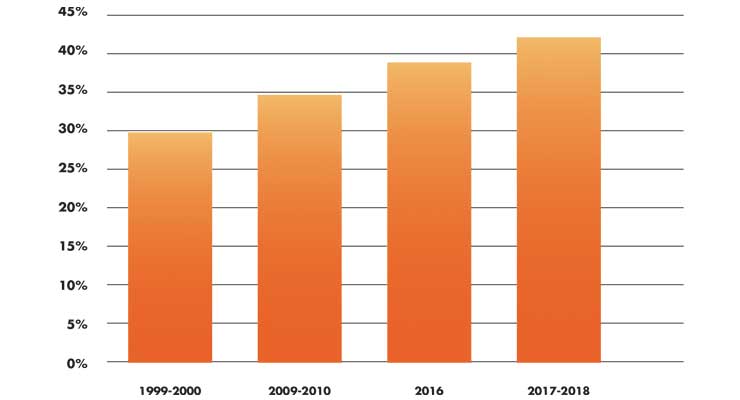
Table 1: Percentage of Obesity in Adults (U.S.)1,2
Why This Is Important
Obesity drives the rate of musculoskeletal disorders, often resulting in hip and knee implants. A large 2016 study (n=2,180) evaluated the impact of body mass index (BMI) in outcomes in primary total knee arthroplasty. Researchers found 93 percent of patients were categorized as overweight or obese. The authors report growing evidence that increasing body mass index, especially in patients with a BMI greater than 40 results in inferior clinical outcomes.5
Obesity-related medical care costs in the United States, in 2008 dollars, were an estimated $147 billion. Annual U.S. productivity costs of obesity-linked absenteeism cover a broad range from $3.38 billion ($79 per obese individual) to $6.38 billion ($132 per individual with obesity).6
Obesity also affects military recruitment. From 2007-2008, 5.7 million men and 16.5 million women who were eligible for military service exceeded the Army’s enlistment standards for weight and body mass index.6
In a clinical study from Lebanon, increased risk of comorbidities was reported for rheumatic and musculoskeletal diseases. In 769 patients, the most common comorbidities were the cardiovascular risk factors and diseases (Table 2)—hypertension (36.5 percent), hypercholesterolemia (30.7 percent), obesity (22.7 percent), smoking (22.1 percent), diabetes (10.4 percent), myocardial infarction (6.6 percent).4
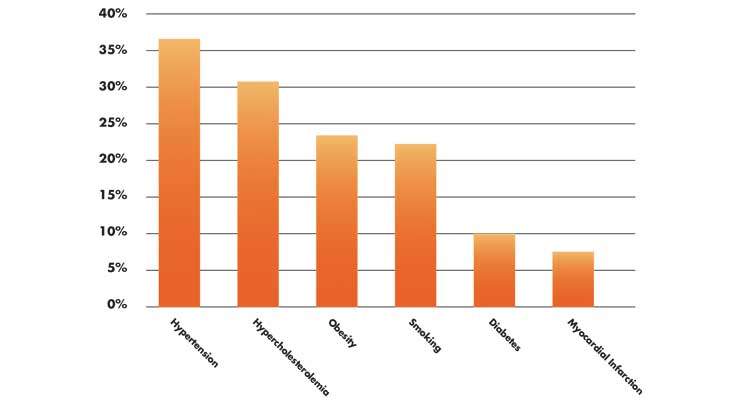
Table 2: Common Comorbidities: Cardiovascular Risk Factors and Diseases4
Before the outbreak of COVID-19, almost 1 million knee replacement procedures were expected to be performed in 2020 in the U.S.7 By 2030, it is projected the number of total knee revisions could total 3.48 million (Table 3).8
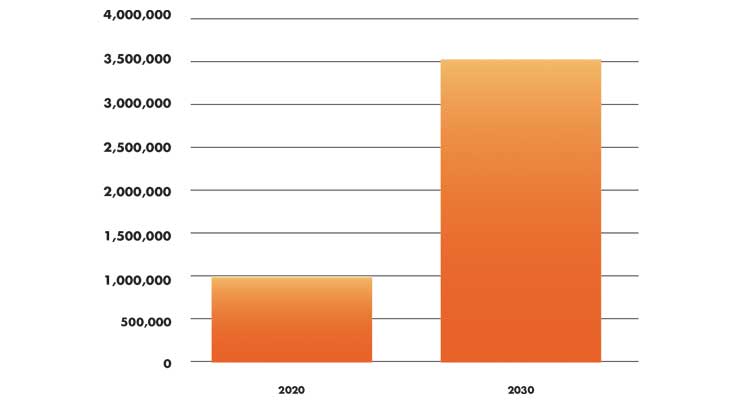
Table 3: Forecasted Growth of Knee Replacement Procedure Rates7,8
Timing is Everything
A January 2020 Northwestern study, published in the Journal of Bone and Joint Surgery (n=8,002), stated that 90 percent of patients with knee osteoarthritis who would benefit from knee replacement surgery are delaying surgery for too long and will see less benefit once they have the procedure. The impact is substantial: Study authors stated waiting too long for surgery causes patients with osteoarthritis to have a deterioration of function. This affects the patient’s ability to walk and exercise, which can exacerbate other conditions such as cardiovascular issues and depression. In addition, patients may not see as much joint function return as compared with a patient who doesn’t wait too long for surgery.7
But are hip and knee implants contraindicated for the obese patient? A 2016 study reviewed 200,054 patient records; 147,691 patients (74 percent) had a recorded BMI. In this study, the mean BMI for patients undergoing total knee arthroplasty was 31kg/m2 (obese). A total of 10,745 patients (16 percent of all obese patients) received implants against manufacturer recommendations that contraindicated the implant due to patient weight.9
A study from The University of Western Australia, published by BMJ, determined overweight and obese patients undergo knee replacements approximately two to eight years earlier than those of normal weight. The scientists found the additional weight produced a pathological tissue modification in the knee, called horizontal fissuring. This is when the space between the bone and cartilage deteriorates, because of increased pressure from obesity.10
The underlying cause of obesity-linked osteoarthritis is complicated and controversial. Atypical mechanical loading and inflammation are factors considered to contribute to the pathogenesis of osteoarthritis.11 Etiology studies of obesity-related osteoarthritis suggest metabolic triggered inflammation is the chief cause of obesity-related osteoarthritis. Other studies suggest osteoarthritis is caused by extreme mechanical loading on articular joints. A population-based study from the Netherlands circulated by the Annals of Rheumatic Diseases also supports the hypothesis that obesity-linked mechanical stress is the most critical risk factor for knee osteoarthritis.11
The Medi-Vantage Perspective
Since the issue of obesity will be with us for the long run, why not develop implants that can reduce the complications associated with obese patients? It will require several years to get a new implant on the market if designing for the specific needs of the obese population. But in a world of commoditized hip and knee implants, doesn’t a goal of a differentiated implant make sense, considering the size of this market segment?
References
Maria Shepherd has more than 20 years of leadership experience in medical device/life-science marketing in small startups and top-tier companies. After her industry career, including her role as vice president of marketing for Oridion Medical where she boosted the company valuation prior to its acquisition by Medtronic, director of marketing for Philips Medical, and senior management roles at Boston Scientific Corp., she founded Medi-Vantage. Medi-Vantage provides marketing and business strategy and innovation research for the medical device industry. The firm quantitatively and qualitatively sizes and segments opportunities, evaluates new technologies, provides marketing services, and performs due diligence for acquisitions. Shepherd has taught marketing and product development courses and can be reached at 617-548-9892 or at mshepherd@medi-vantage. Visit her website at www.medi-vantage.com.
Table 1: Percentage of Obesity in Adults (U.S.)1,2
Why This Is Important
Obesity drives the rate of musculoskeletal disorders, often resulting in hip and knee implants. A large 2016 study (n=2,180) evaluated the impact of body mass index (BMI) in outcomes in primary total knee arthroplasty. Researchers found 93 percent of patients were categorized as overweight or obese. The authors report growing evidence that increasing body mass index, especially in patients with a BMI greater than 40 results in inferior clinical outcomes.5
Obesity-related medical care costs in the United States, in 2008 dollars, were an estimated $147 billion. Annual U.S. productivity costs of obesity-linked absenteeism cover a broad range from $3.38 billion ($79 per obese individual) to $6.38 billion ($132 per individual with obesity).6
Obesity also affects military recruitment. From 2007-2008, 5.7 million men and 16.5 million women who were eligible for military service exceeded the Army’s enlistment standards for weight and body mass index.6
In a clinical study from Lebanon, increased risk of comorbidities was reported for rheumatic and musculoskeletal diseases. In 769 patients, the most common comorbidities were the cardiovascular risk factors and diseases (Table 2)—hypertension (36.5 percent), hypercholesterolemia (30.7 percent), obesity (22.7 percent), smoking (22.1 percent), diabetes (10.4 percent), myocardial infarction (6.6 percent).4
Table 2: Common Comorbidities: Cardiovascular Risk Factors and Diseases4
Before the outbreak of COVID-19, almost 1 million knee replacement procedures were expected to be performed in 2020 in the U.S.7 By 2030, it is projected the number of total knee revisions could total 3.48 million (Table 3).8
Table 3: Forecasted Growth of Knee Replacement Procedure Rates7,8
Timing is Everything
A January 2020 Northwestern study, published in the Journal of Bone and Joint Surgery (n=8,002), stated that 90 percent of patients with knee osteoarthritis who would benefit from knee replacement surgery are delaying surgery for too long and will see less benefit once they have the procedure. The impact is substantial: Study authors stated waiting too long for surgery causes patients with osteoarthritis to have a deterioration of function. This affects the patient’s ability to walk and exercise, which can exacerbate other conditions such as cardiovascular issues and depression. In addition, patients may not see as much joint function return as compared with a patient who doesn’t wait too long for surgery.7
But are hip and knee implants contraindicated for the obese patient? A 2016 study reviewed 200,054 patient records; 147,691 patients (74 percent) had a recorded BMI. In this study, the mean BMI for patients undergoing total knee arthroplasty was 31kg/m2 (obese). A total of 10,745 patients (16 percent of all obese patients) received implants against manufacturer recommendations that contraindicated the implant due to patient weight.9
A study from The University of Western Australia, published by BMJ, determined overweight and obese patients undergo knee replacements approximately two to eight years earlier than those of normal weight. The scientists found the additional weight produced a pathological tissue modification in the knee, called horizontal fissuring. This is when the space between the bone and cartilage deteriorates, because of increased pressure from obesity.10
The underlying cause of obesity-linked osteoarthritis is complicated and controversial. Atypical mechanical loading and inflammation are factors considered to contribute to the pathogenesis of osteoarthritis.11 Etiology studies of obesity-related osteoarthritis suggest metabolic triggered inflammation is the chief cause of obesity-related osteoarthritis. Other studies suggest osteoarthritis is caused by extreme mechanical loading on articular joints. A population-based study from the Netherlands circulated by the Annals of Rheumatic Diseases also supports the hypothesis that obesity-linked mechanical stress is the most critical risk factor for knee osteoarthritis.11
The Medi-Vantage Perspective
Since the issue of obesity will be with us for the long run, why not develop implants that can reduce the complications associated with obese patients? It will require several years to get a new implant on the market if designing for the specific needs of the obese population. But in a world of commoditized hip and knee implants, doesn’t a goal of a differentiated implant make sense, considering the size of this market segment?
References
- bit.ly/odt201101
- bit.ly/odt201102
- bit.ly/odt201103
- bit.ly/odt201104
- bit.ly/odt201105
- bit.ly/odt201106
- bit.ly/odt201107
- bit.ly/odt201108
- bit.ly/odt201109
- bit.ly/odt201110
- bit.ly/odt201111
Maria Shepherd has more than 20 years of leadership experience in medical device/life-science marketing in small startups and top-tier companies. After her industry career, including her role as vice president of marketing for Oridion Medical where she boosted the company valuation prior to its acquisition by Medtronic, director of marketing for Philips Medical, and senior management roles at Boston Scientific Corp., she founded Medi-Vantage. Medi-Vantage provides marketing and business strategy and innovation research for the medical device industry. The firm quantitatively and qualitatively sizes and segments opportunities, evaluates new technologies, provides marketing services, and performs due diligence for acquisitions. Shepherd has taught marketing and product development courses and can be reached at 617-548-9892 or at mshepherd@medi-vantage. Visit her website at www.medi-vantage.com.