Aesculap, the orthopedic unit of German medical device company B. Braun has chosen Invibio
Biomaterial Solutions’ PEEK-Optimacarbon fiber reinforced (CFR) polymer for its EnduRo knee revision system.
Aesculap’s device is 510(k) cleared in the United States by the U.S. Food and Drug Administration (FDA) and also has receive the CE Mark in the European Union. The device was developed to combat the predominant causes of knee implant failure, luxation, wear and poor positioning associated with metal components, Aesculap’s EnduRo knee revision system relies on PEEK-Optima CFR polymer to increase the implant service life and reduce the necessity of subsequent revision surgery, according to Aesculap.
The EnduRo knee is used in the treatment of severe bone defects and ligament insufficiency. It has been commercially available in Europe since January 2010 and U.S. approval came in December 2010. A contributing factor to its fast FDA clearance—within six months of submitting the application—was Invibio’s history withimplantable devices, including the amount of data provided to the submission process, according to the companies.
According to Aesculap, the EnduRo knee has received a strong European marketreception, with 14 percent market share in Germany during the first year of availability and with more than 2,000 prosthesesimplanted to date. The first U.S. implantation of the EnduRo knee was in November 2011.
In 2010, Millennium Research Groupestimated there were more than 90,000 knee revision surgeries performed in the United States and Europe, indicating that approximately 8 percent of all knee implant procedures result from failure of the initial knee implant. A contributing factor to these failures is dislocation, whereby the rotational axis slips out of its guide, requiring total replacement of the implant.
Aesculap claims its knee’s hinge mechanism, joined cone design and the use of PEEK polymer help prevent dislocation compared totraditional hinge mechanism types that use ultra-high-molecular-weight polyethylene. PEEK Optima, however, provides greater wear and cold flow resistance as well asdimensional stability during the lifetime of the device (less than 15 years), which aids resistance to dislocation, according tothe company.
“Aesculap and Invibio have benefited from a long, mutually beneficial relationship based on sharing expertise and knowledge,” said Ulf Grimm, Aesculap’s product manager for Knee Endoprostheses. “It was through technical expertise, an understanding of our requirements and a long history of proven biocompatibility and implantation success that Invibio was able to provide us with an exceptional solution. Throughout this process Invibio has provided valuable processing support and a manufacturing network with the flexibility and scope to meet our device and time targets. Working with Invibio provided us with both a material and processing solution package that enabled our accelerated time to market requirement.”
Knee ReplacementSurgeries Skyrocket
Osteoarthritis has led to a surge in total knee replacement (TKR) surgeries within the last decade, leaving more than 4.5 million Americans living with new knee joints, according to research presented at the 2012 American Academy of Orthopaedic Surgeons Annual Meeting in San Francisco, Calif.
The sharpest rise in TKR patientsoccurred among younger patients, the data showed. Investigators used a computer model, U.S. Census Bureau data, information from the National Health Interview Survey, the Multicenter Osteoarthritis Study and the Osteoarthritis Initiative, as well as other national data and literature to determine the number of U.S. residents living with at least one TKR.
The study found that 4.7 percent of U.S. residents aged 50 and older have undergone TKR, a proportion that is higher than both the national rates for congestive heart failure and rheumatoid arthritis. In addition, the study determined:
- The prevalence of osteoarthritis and TKR is higher in women—5.3 percent of females living with osteoarthritis have had at least one knee replaced, compared with 4.1 percent of men living with the disease and an artificial knee.
- About 4.1 percent of men and 4.8 percent of women aged 60 to 69 have had a TKR. The numbers rise with age: 7.1 percent of men and 8.2 percent of women aged 70 to 79 have had a least one knee replaced.
- Ten percent of Americans aged 80 and older are living with a TKR.
“The number of total knee replacements is growing drastically,” said Elena Losina, Ph.D., lead investigator and co-director of Orthopedic and Arthritis Center for Outcomes Research at Brigham and Women’s Hospital in Boston, Mass. “We now have a lot of people living with TKR.” Such a surge in TKR recipients could lead to substantial increases in future revisions and complications, particularly in younger patients who want to retain their active lifestyles as they age.
The study was funded by the National Institute of Arthritis and Musculoskeletal and Skin Diseases within the U.S. National Institutes of Health. Its findings could help clinicians better understand the future challenges of TKR, including follow-up care, healthcare costs and treatment access.
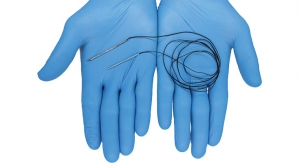
Latest System from Arthrex Combines Three Systems in One
At the risk of sounding a tad metaphysical, life could be viewed as the pursuit of clarity. In medicine—as is the case in many disciplines—a clear view is everything.
Arthrex Inc., a Naples, Fla.-baseddeveloper of arthroscopic and minimally invasive orthopedic surgical technology, pursues this philosophy daily in thecreation of new technology. Recently, the company introduced Synergy HD3 system for the endoscopic market.
The device integrates three components, high-definition cameras, LED lighting and an image management system—all integrated into one console that uses an Apple iPad tablet interface.
Steve Jones, the company’s director of business development characterized the system as “revolutionary,” adding that it “breaks new barriers in endoscopic image management and patient education.”
Before now, according to Jones, the three components that go into theSynergy system have been available only as separate system, which can make the operating room a “cumbersome” place.
The system loads physician preferences and surgical case information. It also can allow authorized viewers to access live streaming videos via the Internet from any location. The iPad application allows the surgeons to review, edit and annotate still images and video recordings that are immediately downloadable. The surgeon also is able to create and transmit customizable documents that he or she could transmit as a post-operative report to patients or other caregivers.
Synergy HD3 is designed and manufactured by the company’s new subsidiary, Arthrex California Technology in Santa Barbara. According to the company, it has developed more than 6,000 products for arthroscopic and minimally invasive surgery. The company has been in growth mode lately. In 2011, the firm hired more than 260 new employees and plans to double its local Florida employment of 1,200 by 2015 to meet demand. The privately held firm says it recorded $1 billion in annual revenue in 2010.
Amedica Has Expanded itsValeo Spinal Line
Amedica Corp. is adding to its stable of spinal products.
The new Valeo VBR (vertebral bodyreplacement) spinal implant is intended for vertebral body replacement to aid in surgical correction and stabilization of the thoracolumbar spine and is designed to restore the biomechanical integrity of the spine. The Valeo VBR will employ the unique material characteristics of the company’s proprietary silicon nitrideceramic, which Amedica officials claim may increase fusion potential in corpectomy procedures (a surgical procedure that involves removing part of the vertebral body—corpus vertebrae, hence the name corpectomy—usually as a way to decompress the spinal cord and nerves.
Corpectomy is often performed in association with some form of discectomy). The company offers a number of cervical and lumbar spacers as part of its Valeo line. Amedica is a spinal and reconstructive implant and instrument manufacturer that is focused on its proprietary siliconnitride ceramic technologies.
“We are excited to offer surgeons yet another option for use of our silicon nitride technology. The availability of this product will result in ease of use for surgeons and potentially better outcomes for patients. This is just one of many future applications that we envision for this unique material,” said Eric Olsen, the company’s recentlyappointed president and CEO.
Amedica’s silicon nitride implants provide a hydrophilic and bone-friendly surface structure that may enhance bone attachment. In addition, the material is fractureresistant and its semi-radiolucent characteristic (easily viewed using standard imaging technology) eases accurate placement,
according to the company.
Olsen also recently told Orthopedic
Design & Technology that silicon nitride may have natural antimicrobial properties that the company continues to explore, along with new applications for the ceramic.
Salt Lake City, Utah-based Amedica is a private equity-backed ceramic manufacturing and implant company founded in 1996. The company is ISO 13485 certified, its spine products are cleared by the U.S. Food and Drug Administration, CE marked in Europe, and sold in ten countries.
In mid-February Amedica completed a recent round of $30 million in financing with the receipt of the final $5,000,000 investment. The proceeds from this financing will be used for further development and distribution of its novel ceramic materials in the orthopedic, spine and dental markets. The proceeds also will be used for payments on debt arising from the U.S. Spine acquisition, and working capital and other corporate purposes. To date, Amedica has raised approximately $140 million.
In September 2010, Amedica acquired privately held U.S. Spine. (See more on the company in the sidebar in this issue’s materials feature.)
New Study Estimates Cost of Defensive Medicine
Data from a new study suggests that defense medicine—and the cost that’s passed on to the healthcare system—is alive and well in orthopedics.
In a first-ever national survey of orthopedic surgeons, 96 percent said they have practiced defensive medicine—the ordering of tests, referrals to specialists and hospital admissions primarily to avoid liability and without significant benefit to patients—according to a new study presented at this year’s annual meeting of the American Academy of Orthopaedic Surgeons (AAOS). The study estimates the annual cost of defensive orthopedic care at $2 billion.
In September 2010, researchers asked 2,000 orthopedic surgeons to complete a Web-based survey on defensive medicine. The orthopedic surgeons were chosen randomly from the AAOS database. Of the 1,214 respondents (61 percent of the total pool), 96 percent responded that they had ordered imaging or laboratory tests, referred patients to specialists, or approved hospital admissions primarily to avoid possible malpractice liability.
More specifically, 24 percent of tests were ordered for defensive reasons: 19 percent of radiography tests, 26 percent of CT scans, 31 percent of MR images and 44 percent of ultrasounds. Participating orthopedic surgeons also acknowledged that defensive medicine was the motivation behind 35 percent of specialist referrals, 23 percent of laboratory tests and 18 percent of biopsies.
Defensive hospital admissions averaged 7 percent each month. Using the average national Medicare payment information from the 2011 Current Procedural Terminology (CPT) code reimbursement data, the cost of defensive medicine per orthopedic surgeon respondent was approximately $8,500 per month or $100,000 per year,representing 24 percent of a physician’sannual spending. Given the U.S. Department of Labor’s statistic of 20,400 practicing orthopedic surgeons in the U.S., investigators estimate the national, annual cost ofdefensive medicine for the specialty of orthopedic surgery at $173 million per month or $2 billion each year.
The study results show that physicians “are clearly concerned about malpractice issues, and they’re adjusting their practice procedures based on that fear,” saidManish K. Sethi, M.D., lead author of the study, and co-director of the VanderbiltOrthopaedic Institute Center for Health Policy. “Eliminating defensive medicine is “an easy thing we can do to lower costs.”
Sethi previously was involved in asimilar study of orthopaedic surgeons in Massachusetts that found comparableresults, but this is the first to demonstrate defensive medicine practices are common throughout the country.
According to Douglas W. Lundy, M.D., F.A.C.S., chairman of the AAOS MedicalLiability Committee said: “Defensive medicine drives up the cost of patient care and limits patient access to specialty care, neither of which are in the interest of our patients who deserve the best and least costly care possible. Unfortunately, the current legal climate forces good doctors to order these tests and practice defensive medicine.”
MedShape Gets Infusion of Cash from GE Capital
The Healthcare Financial Services arm of GE Capital has loaned $3 million to MedShape, Inc. The financing will be used for general working capital purposes, according to a press release issued by both parties.
Headquartered in Atlanta, Ga., MedShape is a privately held medical device company focused on developing orthopedic devices from proprietary shape memory technology. The company is working to build and commercialize a portfolio of surgical solutions that use its patented technologies to address the increasing demand for improved sports medicine, joint fusion and musculoskeletal trauma products.
“As a growing company, we were looking for a lender with deep industry knowledge that could help us meet our business objectives,” said Kurt Jacobus, CEO of MedShape. “The team at GE Capital, Healthcare Financial Services has extensive expertise and worked with us to create a tailored financing solution that will help us execute our growth strategy.”
GE Capital, Healthcare Financial Services has provided more than $60 billion infinancing during the last ten years tocompanies in more than 40 healthcaresectors including senior housing, hospitals, medical offices, outpatient services, pharmaceuticals and medical devices.