Mark Crawford, Contributing Writer05.19.17
Perhaps no other industry has such a locked-in growth market as orthopedic manufacturers do with the retiring baby boomer generation. Boomers have more dispensable income than previous generations, as well as high expectations for active, rewarding post-retirement lifestyles—which means joint replacements for many of them.
“Implant manufacturing continues to grow as more and more baby boomers get their joints replaced,” said David Neal, president and founder of STAT Design LLC, a Morris Plains, N.J.-based orthopedic design and development consulting firm. “Many patients had their devices implanted 20-plus years ago—this group is driving the revision total joint market. The challenge now is to manufacture high-quality implants with the latest technologies, materials, and coatings, while still containing healthcare costs.”
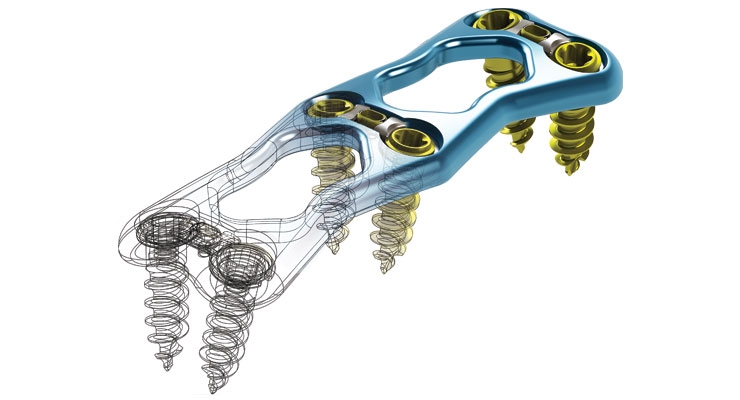
This can indeed be a challenge. Overall, medical device manufacturers (MDMs) are reluctant to change their proven methods and technologies. In order to stay relevant and competitive, however, they must evolve and keep pace with new design strategies and manufacturing techniques, especially additive manufacturing and 3D printing, which have taken hold in spinal implant manufacturing. 3D printing allows engineers to go beyond conventional manufacturing methods to design new implants with pinpoint precision that optimize pore size, porosity, geometry, and surface texture to help promote fusion.
These new design and manufacturing capabilities make the orthopedic market even more competitive and, in some cases, level the playing field somewhat for startups and younger companies with innovative new products.
Despite the growing market for orthopedic products and the exciting new technologies for making them, not every product category is “hot.” Jack Neenan, vice president of sales and business development for Phillips Precision Medicraft, an Elmwood Park, N.J.-based contract manufacturer of advanced orthopedic implants, instrumentation, and sterilization delivery systems, cases, and trays, indicated that large joint implant manufacturing has become commoditized and faces tighter pricing pressures. “In contrast,” he said, “we are seeing more growth in biologics, specialty coatings, and spine and extremity products.”
Other growth markets are minimally invasive surgical procedures and robotic-assisted surgeries.
Many players are looking for new technologies that will make their products the preferred choice of surgeons. They strive to differentiate themselves from their competitors by focusing on products that have value-based results showing reduced time in the operating room or shorter patient recovery times. Sometimes larger OEMs acquire this technology through the buyout of a smaller competitor. There is also a trend toward major OEMs using distribution agreements to gain access to new and innovative products.
“Distribution agreements have really helped some of our smaller customers to private-label their products to the larger OEMs,” said Philip Allen, director of sales and marketing for Lowell, a Minneapolis, Minn.-based contract manufacturer of complex implants for the orthopedic and cardiovascular markets. “The OEMs benefit from innovations added to their product portfolio, without having to make the substantial capital investment needed to acquire the target company.” This also helps keep the supply chain short and reduces regulatory burden, he noted.
When OEMs or startups acquire their new technology or product and come looking for a contract manufacturing organization, “that CMO must have the technical resources to create a benchmark design and manufacture the product in the most cost-effective manner,” said David Cabral, president of Five Star Companies, a New Bedford, Mass.-based orthopedic implant and instrument contract manufacturer specializing in high-precision medical device machining. “Although we have manufactured shoulder implant components for several years, we continue to look for ways to improve upon our processes.”
The orthopedic industry is maturing—especially with its approach for adding value to the healthcare system through its products. “Major OEMs are focusing more on the continuum of care and less on the implant itself,” said Allen. “Implant contract manufacturers work closely with OEMs to make devices that improve a patient’s quality of life, but also reduce the cost of the overall event. Minimally invasive implants lead to faster recovery times and better outcomes. Fewer implant kits lead to less inventory and lower cost. Advances in manufacturing lead to smaller, more complex devices that can be implanted on an outpatient basis, preserve motion, and improve patient satisfaction.”
What OEMs Want
OEMs want higher precision, tighter tolerances, and improved finishes. They seek short lead times, smaller lot quantities, and competitive pricing. They want shorter supply chains, with vendors that can do more as products continually get more complex, including helping with regulatory guidance. Most of all, OEMs demand quality throughout the manufacturing process—not just that the component meets the print, but that equipment and processes are thoroughly validated, traceability is iron-clad, and paperwork is 100-percent accurate.
“Our OEM partners focus on quality and on-time/in-full delivery performance, design for manufacturability (DFM), vendor-managed inventory, and product part approval process,” said Allen.
Time is money, so speed is critical—shorter lifecycles, faster approval, and speedier product release. “Fast turnaround has always been a hot button, but with FDA approval cycles getting longer, lead times have become more crucial to meeting product launch dates,” said Cabral.
Fast turnaround on prototyping is essential for maximizing design for manufacturability (DFM) and creating a smooth, efficient manufacturing process. Now, with 3D printing, prototyping can be accomplished in a matter of days, instead of weeks, greatly accelerating the decision-making process during DFM.
“OEMs are looking for fast and efficient prototyping cycles,” stated John Ruggieri, vice president of engineering and business development for Seabrook Medical, a Seabrook, N.H.-based contract manufacturer of orthopedic implants and instruments. “They also seek strict adherence to manufacturing process capability and repeatability, early DFM engagement, and full service from machining to coatings to packaging, all through a single source.”
Critical time can be saved through more efficient (and less wasteful) processes throughout the product lifecycle. For example, many OEMs are demanding “dock-to-stock” and vendor-managed inventory. OEMs also want agility and flexibility in manufacturing platforms and robust quality assurance/regulatory affairs systems.
“In fact,” said Neenan, “we’ve made a dedicated effort, through lean/5S principles, to adapt our manufacturing operation specifically to meet these needs. By maintaining inventory of select product lines, we’re able to provide our OEMs with an on-demand [no wait time] solution that’s successful in saving many customers time and money.”
As margins grow tighter, OEMs also implement downstream delivery methods to maintain margins and increase sales. For example, novel packaging methods can be used that minimize cost (scrap or waste) in the operating room, or during reprocessing.
“We are seeing a rapid move to disposable, sterile-packed, and surgery-ready instruments, coupled with sterile-packed implants,” said James B. Schultz, executive vice president of sales and marketing for ECA Medical Instruments, a Thousand Oaks, Calif.-based designer and manufacturer of single-procedure torque-limiting surgical instruments, fixed drivers, and customized implant fixation kits. “This bundled model assures 100-percent availability of the implant and instruments, so the OEM never loses a sale waiting for instruments to complete reprocessing and sterilization. This model also promotes reimbursement and new annuity revenue, as the implant company can sell the disposable instrument kits."
Additive Manufacturing/3D Printing
For most orthopedic implant manufacturers, the biggest advantage of 3D printing is prototyping—being able to deliver a functional prototype into the hands of the design team in a matter of hours, instead of days or weeks, made from high-demand materials such as metal and polyether ether ketone (PEEK). A few orthopedic companies have already used 3D printing to build implants that have received 510(k) approval from the U.S. Food and Drug Administration (FDA).
Additive manufacturing is a good choice for implants with low surface-to-volume ratios and implants that have complex geometries, which are difficult to achieve with traditional forging, casting, and machining techniques. In addition, since a variety of materials such as titanium and stainless steel can be used in the additive manufacturing process, functional prototypes can be made out of the same material as production components. This enables more rigorous testing of prototypes while decreasing the development time for new products.
In some cases, 3D printing is being used to build complete orthopedic implants in a single process. This is ideal for low runs, and especially beneficial for one-run, customized, patient-specific products.
More companies are starting to use additive manufacturing/3D printing to make sample and prototype implants. Total joint OEMs are cautious about diving completely into 3D-printed metal parts for production; MDMs of smaller-sized implants, such as those for the spine, foot, and ankle markets, are more aggressive in utilizing this revolutionary manufacturing process. In fact, with tighter tolerances and more complex assemblies associated with implants, engineers are designing products to be manufactured exclusively with 3D printers.
Contract manufacturing organizations (CMOs), too, are in on the action, trying to gently push their resistant OEMs away from subtractive machining processes and toward additive manufacturing for their next-generation implants.
“Additive manufacturing is completely redefining what’s possible to produce in the implants sector,” said Neenan. “It’s exciting to push boundaries, material combinations, and discover new ways to create unique product geometry. We’re seeing trabecular surface structures [which support bone ingrowth] being used more to improve the fixation of these devices—additive manufacturing makes this possible.”
“Orthopedic companies can now rapidly model new implant design concepts into CAD from surgeon input and quickly turn these concepts into physical parts for show-and-tell made with 3D printers,” added Neal. "The iterative design time to produce these rapid plastic prototypes is much shorter compared to traditional manufacturing processes—for example, from typically two to six weeks for traditional machining of metal to less than one week with 3D printing.”
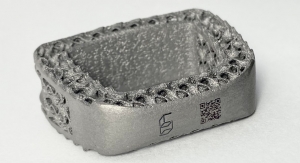
Currently, adjustable spine cages are a hot product for additive manufacturing/3D printing, which allows for the development of porous structures that mimic cancellous bone—a type of spongy bone tissue. This provides spine surgeons with a range of options for addressing their preferences, and meeting the needs of their patients.
Several companies have successfully manufactured spinal implants using 3D printing methods. 4WEB Medical, one of the first MDMs to commercialize 3D-printed spine implants in the United States, recently announced a 3D-printed posterior spine truss system that provides a line of interbody fusion devices, with applications across a wide array of posterior spine procedures. The implants provide functionality such as a biconvex web structure, which distributes the load over a larger surface area at the endplate interface to minimize subsidence.
Orthopedic device behemoth Stryker Corp., which manufactures spinal products for both traditional and minimally invasive surgical procedures, has developed a unique additive manufacturing process that allows the company to create Tritanium—a material with precise porous structures that resemble cancellous bone. Although Tritanium has an organic and randomized appearance, the porous matrix is specifically engineered and controlled by computer models based on studies that revealed which geometries and pore sizes would provide an optimal environment for cells to attach and multiply within the structure.
The first spinal surgery product based on this technology is the Tritanium Posterior Lumbar Cage, an interbody fusion device indicated for use with autograft and/or allogenic bone graft comprised of cancellous and/or corticocancellous bone graft when used as an adjunct to fusion in patients with degenerative disc disease.
Guided by special computer-aided design software, a focused laser beam melts layers of titanium-alloy particles in a process that is repeated hundreds of times, essentially “growing” the device from the bottom up. This gives Stryker the ability to consistently produce precisely engineered porous structures that are difficult or impossible to create using traditional manufacturing processes.
“This ‘precise randomization’ of fully interconnected pores differs from other technologies featuring longitudinal channels and traverse windows that result in a uniform lattice structure, as well as cages offering porosity that is only present on the surface,” said Bradley Paddock, president of Stryker’s Spine division.
The Challenges of Complexity
The ever-increasing tight tolerances required for shapes, features, material bonds, components, and assemblies in complex devices are a constant challenge for CMOs. The more complicated an implant is, the greater the chance something can go wrong. CMOs need to be sure this doesn’t happen—not just to please the OEM, but to be certain that patient safety is not compromised.
“The smaller these devices get, the more we must look at all facets of manufacturing, including sterilization, ease of use, and feasibility of manufacture,” said Cabral.
“One of the big challenges facing designers and the associated implant manufacturer making small and complex devices is strength,” added Neal. “These implants for smaller joints are exposed to high stresses from large forces acting on small contact areas of the mating bearing surfaces, such as that for ankle, elbow, and wrist.”
Another challenge with small, complex devices and assemblies is the communication of design intent so that it survives changes in personnel, manufacturing, and measuring equipment. Lowell, for example, uses high-precision geometric dimensioning and tolerancing (GD&T), the solid model, and 3D model-based drawings to communicate design intent. “It is a common language that reduces errors, miscommunication, and results in lower cost and faster time to market,” said Allen.
Another critical area is tolerance stack-ups in complex assemblies. Stack-ups, which are used to address mechanical fit and performance requirements in assemblies, are often left to the end of the design; if done incorrectly, components may not assemble correctly and the device may not function as designed. “Lowell works closely with our OEM partners to develop robust and manufacturable tolerance schemes that are especially important for smaller and more complex medical devices,” Allen added.
Extremely tight tolerances, and the task of inspecting them, also push manufacturing costs higher. Inspection is a critical step in the manufacturing process that can have a huge impact on quality, safety, and regulatory approval. The design of devices must also be considered from the point of view of inspection; therefore, inspection methods need to be discussed up front during DFM.
“Inspection techniques become increasingly more challenging for both suppliers and OEMs,” said Ruggieri. “Inspection correlation challenges require a substantial effort, and at a very early stage. Most OEMs aren’t ready to tackle the task early enough for their suppliers to be completely successful.”
More implant devices, including combination devices, require the bonding of dissimilar materials to create specific physical characteristics that are critical to performance. These materials may be a challenge to bond together. For example, PEEK is being used more in spine, hip, knee, and shoulder implants because of its strength, light weight, and chemical inertness. PEEK implants can also be coated with hydroxyapatite or titanium to improve bone growth or osseointegration. However, PEEK can be difficult to machine and may also be a problem for coatings.
“Adherence of new coatings can be a challenge with implants, such as titanium applied on PEEK,” said Neal. “Vacuum plasma spray has its thickness and cohesion issues; however, applying titanium with physical vapor deposition can be a good option for addressing these concerns.”
Regulatory Considerations
FDA approval cycles are requiring a longer schedule for completion, which increases the cost pressures for meeting deadlines. OEMs are also asking their CMOs for more information regarding device history records for their legacy products, some of which may be more than 10 years old. “The FDA wants our OEM customers to provide proof of capability, along with traceability, which extends to their subcontractors,” said Neenan. “The transition from ISO 13485:2003 to ISO 13485:2016 is driving this request, as medical device OEMs prepare for compliance no later than May 1, 2019.”
It is important for MDMs to keep in mind that, with smaller implant devices, such as foot, ankle, wrist, and hand, finding a substantially equivalent predicate can be difficult. OEMs tend to rethink their development strategy when no predicate is available, “requiring the expensive and time-consuming FDA premarket approval (PMA) route over the 510(k) release,” said Neal. “This must all be factored into the project ROI, as a 510(k) application costs around $5,000 and takes about 90 days to clear, compared to a PMA clearance that costs $250,000 plus the costs of a clinical trial, which can take years.”
Moving Forward
Implant designers and engineers are excited to add more functionality to their products, improve outcomes, control costs, and gain market share by using additive manufacturing and 3D printing. Technology (or the combination of technologies) has reached the point where designs that were once impossible to consider can now be made, resulting in improved patient experiences. With the combination of additive manufacturing and special CAD software, such as nTopology, porous structures can be added to implant designs. Parts can be built as a one-piece construction rather than fusing components together—a labor-intensive process that is more prone to error. Additive manufacturing can even produce hollowed-out (shelled) parts, thereby lightening the part in areas where strength is needed less, saving money due to the use of fewer raw materials. Implant concepts can be developed and shown to doctors for review in a matter of days, rather than weeks.
Further, sophisticated 3D printers are also coming down in price, making them affordable for just about any OEM/CMO budget. “Smaller companies can now purchase their own 3D printers with a decent build volume and a 20 to 100 micron (0.0008 inch to 0.004 inch) layer resolution level, for less than a $5,000 investment,” said Neal.
“With the technologies and processes we have at hand, we often surprise our OEMs with a solution or design modification they did not expect, or did not consider, that results in a meaningful benefit for them,” said Neenan. “Our engineers have hands-on machining experience, which allows us to provide a uniquely thorough design for manufacturability. This has a direct effect on how we approach refining a design and a manufacturing process (including additive), or creating custom tooling to maximize production efficiencies. This generally results in improved functionality, lower cost, and faster time to market—increasingly important as medical implants become smaller and more complex.”
Mark Crawford is a full-time freelance business and marketing/communications writer based in Madison, Wis. His clients range from startups to global manufacturing leaders. He also writes a variety of feature articles for regional and national publications and is the author of five books.
“Implant manufacturing continues to grow as more and more baby boomers get their joints replaced,” said David Neal, president and founder of STAT Design LLC, a Morris Plains, N.J.-based orthopedic design and development consulting firm. “Many patients had their devices implanted 20-plus years ago—this group is driving the revision total joint market. The challenge now is to manufacture high-quality implants with the latest technologies, materials, and coatings, while still containing healthcare costs.”
This can indeed be a challenge. Overall, medical device manufacturers (MDMs) are reluctant to change their proven methods and technologies. In order to stay relevant and competitive, however, they must evolve and keep pace with new design strategies and manufacturing techniques, especially additive manufacturing and 3D printing, which have taken hold in spinal implant manufacturing. 3D printing allows engineers to go beyond conventional manufacturing methods to design new implants with pinpoint precision that optimize pore size, porosity, geometry, and surface texture to help promote fusion.
These new design and manufacturing capabilities make the orthopedic market even more competitive and, in some cases, level the playing field somewhat for startups and younger companies with innovative new products.
Despite the growing market for orthopedic products and the exciting new technologies for making them, not every product category is “hot.” Jack Neenan, vice president of sales and business development for Phillips Precision Medicraft, an Elmwood Park, N.J.-based contract manufacturer of advanced orthopedic implants, instrumentation, and sterilization delivery systems, cases, and trays, indicated that large joint implant manufacturing has become commoditized and faces tighter pricing pressures. “In contrast,” he said, “we are seeing more growth in biologics, specialty coatings, and spine and extremity products.”
Other growth markets are minimally invasive surgical procedures and robotic-assisted surgeries.
Many players are looking for new technologies that will make their products the preferred choice of surgeons. They strive to differentiate themselves from their competitors by focusing on products that have value-based results showing reduced time in the operating room or shorter patient recovery times. Sometimes larger OEMs acquire this technology through the buyout of a smaller competitor. There is also a trend toward major OEMs using distribution agreements to gain access to new and innovative products.
“Distribution agreements have really helped some of our smaller customers to private-label their products to the larger OEMs,” said Philip Allen, director of sales and marketing for Lowell, a Minneapolis, Minn.-based contract manufacturer of complex implants for the orthopedic and cardiovascular markets. “The OEMs benefit from innovations added to their product portfolio, without having to make the substantial capital investment needed to acquire the target company.” This also helps keep the supply chain short and reduces regulatory burden, he noted.
When OEMs or startups acquire their new technology or product and come looking for a contract manufacturing organization, “that CMO must have the technical resources to create a benchmark design and manufacture the product in the most cost-effective manner,” said David Cabral, president of Five Star Companies, a New Bedford, Mass.-based orthopedic implant and instrument contract manufacturer specializing in high-precision medical device machining. “Although we have manufactured shoulder implant components for several years, we continue to look for ways to improve upon our processes.”
The orthopedic industry is maturing—especially with its approach for adding value to the healthcare system through its products. “Major OEMs are focusing more on the continuum of care and less on the implant itself,” said Allen. “Implant contract manufacturers work closely with OEMs to make devices that improve a patient’s quality of life, but also reduce the cost of the overall event. Minimally invasive implants lead to faster recovery times and better outcomes. Fewer implant kits lead to less inventory and lower cost. Advances in manufacturing lead to smaller, more complex devices that can be implanted on an outpatient basis, preserve motion, and improve patient satisfaction.”
What OEMs Want
OEMs want higher precision, tighter tolerances, and improved finishes. They seek short lead times, smaller lot quantities, and competitive pricing. They want shorter supply chains, with vendors that can do more as products continually get more complex, including helping with regulatory guidance. Most of all, OEMs demand quality throughout the manufacturing process—not just that the component meets the print, but that equipment and processes are thoroughly validated, traceability is iron-clad, and paperwork is 100-percent accurate.
“Our OEM partners focus on quality and on-time/in-full delivery performance, design for manufacturability (DFM), vendor-managed inventory, and product part approval process,” said Allen.
Time is money, so speed is critical—shorter lifecycles, faster approval, and speedier product release. “Fast turnaround has always been a hot button, but with FDA approval cycles getting longer, lead times have become more crucial to meeting product launch dates,” said Cabral.
Fast turnaround on prototyping is essential for maximizing design for manufacturability (DFM) and creating a smooth, efficient manufacturing process. Now, with 3D printing, prototyping can be accomplished in a matter of days, instead of weeks, greatly accelerating the decision-making process during DFM.
“OEMs are looking for fast and efficient prototyping cycles,” stated John Ruggieri, vice president of engineering and business development for Seabrook Medical, a Seabrook, N.H.-based contract manufacturer of orthopedic implants and instruments. “They also seek strict adherence to manufacturing process capability and repeatability, early DFM engagement, and full service from machining to coatings to packaging, all through a single source.”
Critical time can be saved through more efficient (and less wasteful) processes throughout the product lifecycle. For example, many OEMs are demanding “dock-to-stock” and vendor-managed inventory. OEMs also want agility and flexibility in manufacturing platforms and robust quality assurance/regulatory affairs systems.
“In fact,” said Neenan, “we’ve made a dedicated effort, through lean/5S principles, to adapt our manufacturing operation specifically to meet these needs. By maintaining inventory of select product lines, we’re able to provide our OEMs with an on-demand [no wait time] solution that’s successful in saving many customers time and money.”
As margins grow tighter, OEMs also implement downstream delivery methods to maintain margins and increase sales. For example, novel packaging methods can be used that minimize cost (scrap or waste) in the operating room, or during reprocessing.
“We are seeing a rapid move to disposable, sterile-packed, and surgery-ready instruments, coupled with sterile-packed implants,” said James B. Schultz, executive vice president of sales and marketing for ECA Medical Instruments, a Thousand Oaks, Calif.-based designer and manufacturer of single-procedure torque-limiting surgical instruments, fixed drivers, and customized implant fixation kits. “This bundled model assures 100-percent availability of the implant and instruments, so the OEM never loses a sale waiting for instruments to complete reprocessing and sterilization. This model also promotes reimbursement and new annuity revenue, as the implant company can sell the disposable instrument kits."
Additive Manufacturing/3D Printing
For most orthopedic implant manufacturers, the biggest advantage of 3D printing is prototyping—being able to deliver a functional prototype into the hands of the design team in a matter of hours, instead of days or weeks, made from high-demand materials such as metal and polyether ether ketone (PEEK). A few orthopedic companies have already used 3D printing to build implants that have received 510(k) approval from the U.S. Food and Drug Administration (FDA).
Additive manufacturing is a good choice for implants with low surface-to-volume ratios and implants that have complex geometries, which are difficult to achieve with traditional forging, casting, and machining techniques. In addition, since a variety of materials such as titanium and stainless steel can be used in the additive manufacturing process, functional prototypes can be made out of the same material as production components. This enables more rigorous testing of prototypes while decreasing the development time for new products.
In some cases, 3D printing is being used to build complete orthopedic implants in a single process. This is ideal for low runs, and especially beneficial for one-run, customized, patient-specific products.
More companies are starting to use additive manufacturing/3D printing to make sample and prototype implants. Total joint OEMs are cautious about diving completely into 3D-printed metal parts for production; MDMs of smaller-sized implants, such as those for the spine, foot, and ankle markets, are more aggressive in utilizing this revolutionary manufacturing process. In fact, with tighter tolerances and more complex assemblies associated with implants, engineers are designing products to be manufactured exclusively with 3D printers.
Contract manufacturing organizations (CMOs), too, are in on the action, trying to gently push their resistant OEMs away from subtractive machining processes and toward additive manufacturing for their next-generation implants.
“Additive manufacturing is completely redefining what’s possible to produce in the implants sector,” said Neenan. “It’s exciting to push boundaries, material combinations, and discover new ways to create unique product geometry. We’re seeing trabecular surface structures [which support bone ingrowth] being used more to improve the fixation of these devices—additive manufacturing makes this possible.”
“Orthopedic companies can now rapidly model new implant design concepts into CAD from surgeon input and quickly turn these concepts into physical parts for show-and-tell made with 3D printers,” added Neal. "The iterative design time to produce these rapid plastic prototypes is much shorter compared to traditional manufacturing processes—for example, from typically two to six weeks for traditional machining of metal to less than one week with 3D printing.”
Currently, adjustable spine cages are a hot product for additive manufacturing/3D printing, which allows for the development of porous structures that mimic cancellous bone—a type of spongy bone tissue. This provides spine surgeons with a range of options for addressing their preferences, and meeting the needs of their patients.
Several companies have successfully manufactured spinal implants using 3D printing methods. 4WEB Medical, one of the first MDMs to commercialize 3D-printed spine implants in the United States, recently announced a 3D-printed posterior spine truss system that provides a line of interbody fusion devices, with applications across a wide array of posterior spine procedures. The implants provide functionality such as a biconvex web structure, which distributes the load over a larger surface area at the endplate interface to minimize subsidence.
Orthopedic device behemoth Stryker Corp., which manufactures spinal products for both traditional and minimally invasive surgical procedures, has developed a unique additive manufacturing process that allows the company to create Tritanium—a material with precise porous structures that resemble cancellous bone. Although Tritanium has an organic and randomized appearance, the porous matrix is specifically engineered and controlled by computer models based on studies that revealed which geometries and pore sizes would provide an optimal environment for cells to attach and multiply within the structure.
The first spinal surgery product based on this technology is the Tritanium Posterior Lumbar Cage, an interbody fusion device indicated for use with autograft and/or allogenic bone graft comprised of cancellous and/or corticocancellous bone graft when used as an adjunct to fusion in patients with degenerative disc disease.
Guided by special computer-aided design software, a focused laser beam melts layers of titanium-alloy particles in a process that is repeated hundreds of times, essentially “growing” the device from the bottom up. This gives Stryker the ability to consistently produce precisely engineered porous structures that are difficult or impossible to create using traditional manufacturing processes.
“This ‘precise randomization’ of fully interconnected pores differs from other technologies featuring longitudinal channels and traverse windows that result in a uniform lattice structure, as well as cages offering porosity that is only present on the surface,” said Bradley Paddock, president of Stryker’s Spine division.
The Challenges of Complexity
The ever-increasing tight tolerances required for shapes, features, material bonds, components, and assemblies in complex devices are a constant challenge for CMOs. The more complicated an implant is, the greater the chance something can go wrong. CMOs need to be sure this doesn’t happen—not just to please the OEM, but to be certain that patient safety is not compromised.
“The smaller these devices get, the more we must look at all facets of manufacturing, including sterilization, ease of use, and feasibility of manufacture,” said Cabral.
“One of the big challenges facing designers and the associated implant manufacturer making small and complex devices is strength,” added Neal. “These implants for smaller joints are exposed to high stresses from large forces acting on small contact areas of the mating bearing surfaces, such as that for ankle, elbow, and wrist.”
Another challenge with small, complex devices and assemblies is the communication of design intent so that it survives changes in personnel, manufacturing, and measuring equipment. Lowell, for example, uses high-precision geometric dimensioning and tolerancing (GD&T), the solid model, and 3D model-based drawings to communicate design intent. “It is a common language that reduces errors, miscommunication, and results in lower cost and faster time to market,” said Allen.
Another critical area is tolerance stack-ups in complex assemblies. Stack-ups, which are used to address mechanical fit and performance requirements in assemblies, are often left to the end of the design; if done incorrectly, components may not assemble correctly and the device may not function as designed. “Lowell works closely with our OEM partners to develop robust and manufacturable tolerance schemes that are especially important for smaller and more complex medical devices,” Allen added.
Extremely tight tolerances, and the task of inspecting them, also push manufacturing costs higher. Inspection is a critical step in the manufacturing process that can have a huge impact on quality, safety, and regulatory approval. The design of devices must also be considered from the point of view of inspection; therefore, inspection methods need to be discussed up front during DFM.
“Inspection techniques become increasingly more challenging for both suppliers and OEMs,” said Ruggieri. “Inspection correlation challenges require a substantial effort, and at a very early stage. Most OEMs aren’t ready to tackle the task early enough for their suppliers to be completely successful.”
More implant devices, including combination devices, require the bonding of dissimilar materials to create specific physical characteristics that are critical to performance. These materials may be a challenge to bond together. For example, PEEK is being used more in spine, hip, knee, and shoulder implants because of its strength, light weight, and chemical inertness. PEEK implants can also be coated with hydroxyapatite or titanium to improve bone growth or osseointegration. However, PEEK can be difficult to machine and may also be a problem for coatings.
“Adherence of new coatings can be a challenge with implants, such as titanium applied on PEEK,” said Neal. “Vacuum plasma spray has its thickness and cohesion issues; however, applying titanium with physical vapor deposition can be a good option for addressing these concerns.”
Regulatory Considerations
FDA approval cycles are requiring a longer schedule for completion, which increases the cost pressures for meeting deadlines. OEMs are also asking their CMOs for more information regarding device history records for their legacy products, some of which may be more than 10 years old. “The FDA wants our OEM customers to provide proof of capability, along with traceability, which extends to their subcontractors,” said Neenan. “The transition from ISO 13485:2003 to ISO 13485:2016 is driving this request, as medical device OEMs prepare for compliance no later than May 1, 2019.”
It is important for MDMs to keep in mind that, with smaller implant devices, such as foot, ankle, wrist, and hand, finding a substantially equivalent predicate can be difficult. OEMs tend to rethink their development strategy when no predicate is available, “requiring the expensive and time-consuming FDA premarket approval (PMA) route over the 510(k) release,” said Neal. “This must all be factored into the project ROI, as a 510(k) application costs around $5,000 and takes about 90 days to clear, compared to a PMA clearance that costs $250,000 plus the costs of a clinical trial, which can take years.”
Moving Forward
Implant designers and engineers are excited to add more functionality to their products, improve outcomes, control costs, and gain market share by using additive manufacturing and 3D printing. Technology (or the combination of technologies) has reached the point where designs that were once impossible to consider can now be made, resulting in improved patient experiences. With the combination of additive manufacturing and special CAD software, such as nTopology, porous structures can be added to implant designs. Parts can be built as a one-piece construction rather than fusing components together—a labor-intensive process that is more prone to error. Additive manufacturing can even produce hollowed-out (shelled) parts, thereby lightening the part in areas where strength is needed less, saving money due to the use of fewer raw materials. Implant concepts can be developed and shown to doctors for review in a matter of days, rather than weeks.
Further, sophisticated 3D printers are also coming down in price, making them affordable for just about any OEM/CMO budget. “Smaller companies can now purchase their own 3D printers with a decent build volume and a 20 to 100 micron (0.0008 inch to 0.004 inch) layer resolution level, for less than a $5,000 investment,” said Neal.
“With the technologies and processes we have at hand, we often surprise our OEMs with a solution or design modification they did not expect, or did not consider, that results in a meaningful benefit for them,” said Neenan. “Our engineers have hands-on machining experience, which allows us to provide a uniquely thorough design for manufacturability. This has a direct effect on how we approach refining a design and a manufacturing process (including additive), or creating custom tooling to maximize production efficiencies. This generally results in improved functionality, lower cost, and faster time to market—increasingly important as medical implants become smaller and more complex.”
Mark Crawford is a full-time freelance business and marketing/communications writer based in Madison, Wis. His clients range from startups to global manufacturing leaders. He also writes a variety of feature articles for regional and national publications and is the author of five books.