Robert N. Steensen, MD, Orthopedic One08.04.23
Total knee arthroplasty (TKA) has been a successful procedure for decades and has improved many patients’ lives. Yet about 20% of patients are unsatisfied with their result. A total knee replacement tries to duplicate the function of the knee by creating alignment, balance (medial-lateral), and stability (anterior-posterior). There are several philosophies and, therefore, several techniques to accomplish these goals. The traditional procedure—mechanical alignment (MA)—makes neutral alignment its goal. It creates a straight line from hip to knee to ankle with a perpendicular joint line. Balance is achieved by releasing ligaments if necessary.
Stability is a function of the implant and how the posterior cruciate ligament (PCL) is managed. But as time progressed, technology advanced and patient-specific instrumentation, navigation, and robotics became available. In many cases, these enhanced, more expensive technologies attempt to produce more precise mechanical alignment by decreasing the margin of error. Studies show they were more successful in achieving the alignment goal but did not improve clinical outcomes. Thus, the question becomes: How can the orthopedic industry (and hospitals) justify the increased cost of these procedures if they do not improve the outcomes?
In recent years, there has been consideration of alternative alignment strategies to improve patient satisfaction. These strategies have assumed many labels: kinematic alignment (KA), inverse kinematic alignment (iKA), anatomic alignment (AA), and functional alignment (FA). This article will examine the underlying goals of these alternative alignment strategies.
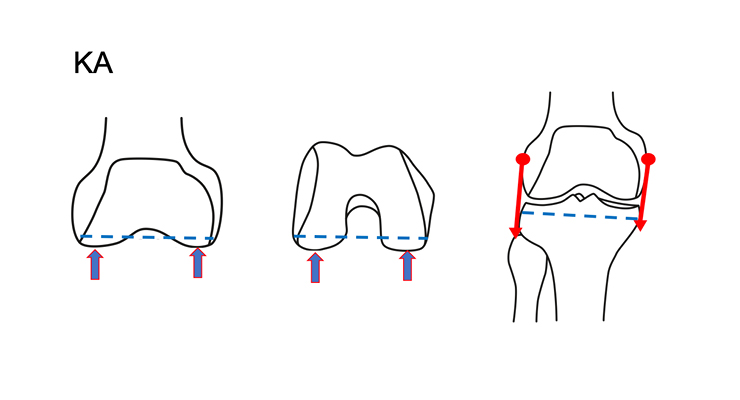
Kinematic alignment attempts to restore the natural, pre-arthritic joint line (Figure 1). With this technique, the patient’s alignment is not restored to an arbitrary goal, but rather to the individual, pre-wear alignment.
Placing the femoral and tibial surfaces in the original position restores normal ligament tension. KA prioritizes the femoral surface because the tibia and patella rotate about the femur. This approach will align the knee’s flexion-extension axis. There are two camps within kinematic alignment, restricted and unrestricted. The restricted group limits the femoral and tibial resection angles. Surgeons using this approach correct for wear and in some cases, excessive deformity.
Conversely, unrestricted kinematic alignment corrects for wear only and accepts the patients’ pre-arthritic anatomy. Most patients are treated the same by restricted and unrestricted kinematic alignment technique, except for far outliers.
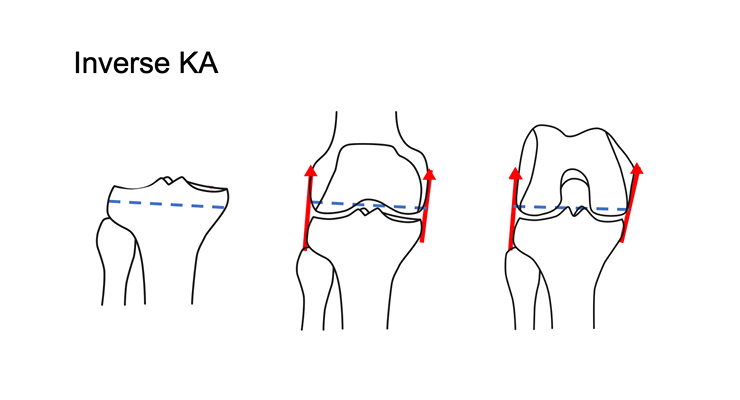
Inverse kinematic alignment focuses on the tibial surface (Figure 2). Using this approach, surgeons match the tibial surface and then base the distal and posterior femoral cuts from the tibial resection. The tibial surface is more difficult to reference because of its varied topography and higher susceptibility to excessive wear. Gap balancing is performed from the presumed native tibial joint line.
Anatomic alignment emerged years ago with the goal of creating the same straight hip-knee-ankle angle as MA but with the joint line at a more natural 3 degrees of varus. Alignment is not individualized and some ligament releases may be needed.
Functional alignment, on the other hand, uses robotic technology to adjust the implant position to achieve equal extension and flexion gaps. The extension gap is similar to a restricted KA approach, while the flexion gap is similar to a gap balance MA approach, often at 3 degrees of external rotation, but these are individualized.
There is a wide variation in natural knee alignment. A bell-shaped curve can represent limb alignment distribution. Recently Hirschmann et. al, introduced the concept of knee phenotypes, suggesting that even knees with the same alignment may not be the same. A knee’s alignment is created by three factors: the distal femoral angle, the proximal tibial angle, and the angle created by cartilage loss. Mechanical alignment and anatomic alignment attempt to narrow the bell-shaped curve as much as possible by trying to make each leg straight. Kinematic alignment attempts to narrow the curve only by the angle created by cartilage loss, while preserving the natural femoral and tibial angles and natural extension and flexion gaps. Functional alignment creates individualized balanced extension and flexion gaps.
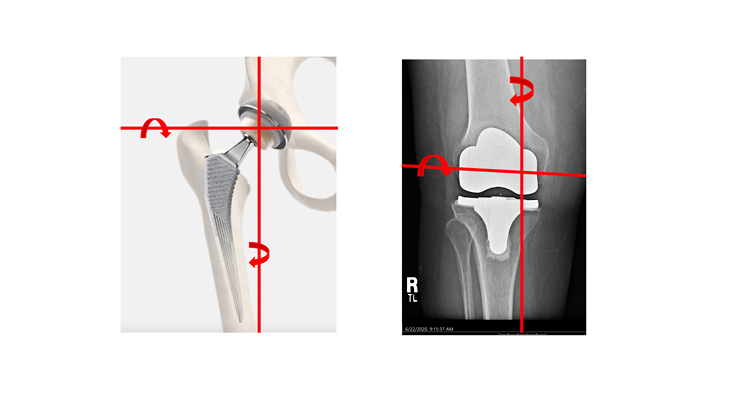
It is commonly thought that total hip replacement patients recover faster and are more satisfied than total knee replacement patients. The nature of total hip replacement replicates the joint’s natural center of rotation. Traditional mechanical TKA alignment does not match the knee’s flexion-extension axis, and traditional cruciate retaining or posterior stabilized implants do not match the knee’s rotational axis. Combining kinematic alignment and a medial pivot implant restores the knee’s flexion-extension axis and its rotational axis. (Figure 3).
Enhanced technology such as navigation and robotics help improve alignment precision. When that precision was used to achieve mechanical alignment, it did not improve patient outcomes suggesting mechanical alignment is not the goal. Technology is now being adapted to alternative alignment techniques, but these methods are not always principle-based.
If alignment is the primary goal, MA or AA are designed to achieve a straight limb, but ligament releases may be necessary. MA has resulted in an 80% patient satisfaction rate. KA can replicate natural limb alignment and ligament balance, including a balanced extension gap and a natural flexion gap (with very slight lateral opening). If a balanced extension and flexion gap are desired, FA can be utilized, and the flexion gap will be balanced but tighter than natural.
Technological advances are not limited to computer navigation and robotics but can be a re-design of manual instruments. An example is the MicroPort Kinematic Alignment Set, which allows measurement of cartilage thickness to determine wear, and the femoral guide adjusts resections to restore the native joint line. Once the femoral surface has been restored, one measures the resection of the tibia needed to balance the knee in extension, and a dual stylus, variable angle tibial guide sets the medial and lateral resections.
Total knee arthroplasty is, and has been, a great advance in patient care. It is paramount to consider technology as a tool to perform a principle-based approach. Technology can assist in achieving goals, but the philosophy and goals must guide the use of technology. Whether a surgeon uses advanced manual instruments or navigation or robotics, the technique will drive patient outcomes.
[Disclosure: Dr. Steensen is a consultant for and receives royalties from MicroPort Orthopedics.]
Robert Steensen, M.D., FAAOS, has practiced in Columbus, Ohio, for more than 30 years. He is faculty at the Orthopedic Surgery Residency at Mount Carmel Health System, the second-largest healthcare system in Central Ohio. He is a partner in Orthopedic One, the largest private practice orthopedic group in the state of Ohio. He has won awards from the American Academy of Orthopaedic Surgeons and the Orthopedic Research Society. Dr. Steensen designed the MicroPort KA Instrument Set and has special interest in knee alignment and in patellar dislocation.
Stability is a function of the implant and how the posterior cruciate ligament (PCL) is managed. But as time progressed, technology advanced and patient-specific instrumentation, navigation, and robotics became available. In many cases, these enhanced, more expensive technologies attempt to produce more precise mechanical alignment by decreasing the margin of error. Studies show they were more successful in achieving the alignment goal but did not improve clinical outcomes. Thus, the question becomes: How can the orthopedic industry (and hospitals) justify the increased cost of these procedures if they do not improve the outcomes?
In recent years, there has been consideration of alternative alignment strategies to improve patient satisfaction. These strategies have assumed many labels: kinematic alignment (KA), inverse kinematic alignment (iKA), anatomic alignment (AA), and functional alignment (FA). This article will examine the underlying goals of these alternative alignment strategies.
Kinematic alignment attempts to restore the natural, pre-arthritic joint line (Figure 1). With this technique, the patient’s alignment is not restored to an arbitrary goal, but rather to the individual, pre-wear alignment.
Placing the femoral and tibial surfaces in the original position restores normal ligament tension. KA prioritizes the femoral surface because the tibia and patella rotate about the femur. This approach will align the knee’s flexion-extension axis. There are two camps within kinematic alignment, restricted and unrestricted. The restricted group limits the femoral and tibial resection angles. Surgeons using this approach correct for wear and in some cases, excessive deformity.
Conversely, unrestricted kinematic alignment corrects for wear only and accepts the patients’ pre-arthritic anatomy. Most patients are treated the same by restricted and unrestricted kinematic alignment technique, except for far outliers.
Inverse kinematic alignment focuses on the tibial surface (Figure 2). Using this approach, surgeons match the tibial surface and then base the distal and posterior femoral cuts from the tibial resection. The tibial surface is more difficult to reference because of its varied topography and higher susceptibility to excessive wear. Gap balancing is performed from the presumed native tibial joint line.
Anatomic alignment emerged years ago with the goal of creating the same straight hip-knee-ankle angle as MA but with the joint line at a more natural 3 degrees of varus. Alignment is not individualized and some ligament releases may be needed.
Functional alignment, on the other hand, uses robotic technology to adjust the implant position to achieve equal extension and flexion gaps. The extension gap is similar to a restricted KA approach, while the flexion gap is similar to a gap balance MA approach, often at 3 degrees of external rotation, but these are individualized.
There is a wide variation in natural knee alignment. A bell-shaped curve can represent limb alignment distribution. Recently Hirschmann et. al, introduced the concept of knee phenotypes, suggesting that even knees with the same alignment may not be the same. A knee’s alignment is created by three factors: the distal femoral angle, the proximal tibial angle, and the angle created by cartilage loss. Mechanical alignment and anatomic alignment attempt to narrow the bell-shaped curve as much as possible by trying to make each leg straight. Kinematic alignment attempts to narrow the curve only by the angle created by cartilage loss, while preserving the natural femoral and tibial angles and natural extension and flexion gaps. Functional alignment creates individualized balanced extension and flexion gaps.
It is commonly thought that total hip replacement patients recover faster and are more satisfied than total knee replacement patients. The nature of total hip replacement replicates the joint’s natural center of rotation. Traditional mechanical TKA alignment does not match the knee’s flexion-extension axis, and traditional cruciate retaining or posterior stabilized implants do not match the knee’s rotational axis. Combining kinematic alignment and a medial pivot implant restores the knee’s flexion-extension axis and its rotational axis. (Figure 3).
Enhanced technology such as navigation and robotics help improve alignment precision. When that precision was used to achieve mechanical alignment, it did not improve patient outcomes suggesting mechanical alignment is not the goal. Technology is now being adapted to alternative alignment techniques, but these methods are not always principle-based.
If alignment is the primary goal, MA or AA are designed to achieve a straight limb, but ligament releases may be necessary. MA has resulted in an 80% patient satisfaction rate. KA can replicate natural limb alignment and ligament balance, including a balanced extension gap and a natural flexion gap (with very slight lateral opening). If a balanced extension and flexion gap are desired, FA can be utilized, and the flexion gap will be balanced but tighter than natural.
Technological advances are not limited to computer navigation and robotics but can be a re-design of manual instruments. An example is the MicroPort Kinematic Alignment Set, which allows measurement of cartilage thickness to determine wear, and the femoral guide adjusts resections to restore the native joint line. Once the femoral surface has been restored, one measures the resection of the tibia needed to balance the knee in extension, and a dual stylus, variable angle tibial guide sets the medial and lateral resections.
Total knee arthroplasty is, and has been, a great advance in patient care. It is paramount to consider technology as a tool to perform a principle-based approach. Technology can assist in achieving goals, but the philosophy and goals must guide the use of technology. Whether a surgeon uses advanced manual instruments or navigation or robotics, the technique will drive patient outcomes.
[Disclosure: Dr. Steensen is a consultant for and receives royalties from MicroPort Orthopedics.]
Robert Steensen, M.D., FAAOS, has practiced in Columbus, Ohio, for more than 30 years. He is faculty at the Orthopedic Surgery Residency at Mount Carmel Health System, the second-largest healthcare system in Central Ohio. He is a partner in Orthopedic One, the largest private practice orthopedic group in the state of Ohio. He has won awards from the American Academy of Orthopaedic Surgeons and the Orthopedic Research Society. Dr. Steensen designed the MicroPort KA Instrument Set and has special interest in knee alignment and in patellar dislocation.
