Michael Barbella, Managing Editor11.13.23
The world finally woke from its long, dreadful nightmare this year.
Forty months after declaring the SARS-CoV-2 virus a global threat, WHO’s director-general officially ended the COVID-19 public health emergency on May 11. “For more than a year, the pandemic has been on a downward trend…” Tedros Adhanom Ghebreyesus stated at a media briefing in Geneva. “This trend has allowed most countries to return to life as we knew it before COVID-19. It is therefore with great hope that I declare COVID-19 over as a global health emergency.”
Free at last.
Free with a caveat, actually: Although the global health emergency is over, the pandemic itself is still public threat, Adhanom Ghebreyesus warned, virulent enough to claim a life every three minutes and savvy enough to evade extinction via perpetual mutations.
So the pandemic continues. And, as history has repeatedly proven, it probably will continue for quite some time. Pandemics seldom have clean conclusions; their endings tend to be ragged and messy—similar to life itself. Some return repeatedly before fading (the Black Death reappeared more than 40 times over 400 years), while others never completely go away.
COVID-19 will likely become one of those everlasting nuisances, lurking in the shadows to disrupt life every once in a while. The world now has to adjust to its new normal.
It won’t be easy. “As we have seen time and time again throughout human history,” a Time commentary reminded readers, “pandemics do not end—they echo.”
Better get used to the reverberation.
That is the advice Helena Holma is offering to startups and rookie entrepreneurs intimidated by the new Medical Device Regulation (MDR). “If you are a startup within healthtech—embrace the regulations,” Holma wrote in an early January blog. “There is no way around them and even if they may seem discouraging, remember they are for a good cause—to ensure patient safety and privacy. If you are well familiar with the regulations and include them in your business strategy, it will give you a competitive advantage.”
Perhaps, but MDR compliance is actually more of a necessity these days as Europe transitions to its long-awaited, much-debated, widely-hated medical device certification rules. Implemented in May 2017, European lawmakers drafted the MDR to update the continent’s archaic Medical Device Directive and harmonize the regulatory review and product approval process across all EU member states.
Although the medtech industry lauded the modernized rules—hopeful they would foster more patient-oriented innovation and better support the specific needs of small and medium-sized enterprises—manufacturers took issue with the MDR’s final compliance deadline, contending the three-year window was “unrealistic” and would lead to widespread device shortages. Calls for a deadline extension intensified as the May 26, 2020, due date approached, though the industry received an unexpected (but nevertheless welcome) one-year reprieve courtesy of COVID-19.
Since then, a growing chorus of industry groups and medtech firms have clamored for an extension to the MDR’s May 26, 2024, re-certification deadline, citing massive Notified Body backlogs and protracted reauthorization waits. As of March (2023), those waits averaged anywhere from six to 23 months (for QMS+product certification applications), while authorization requests nearly doubled, going from 6,188 in April 2022 to 11,418 in March 2023, European Commission survey data indicate.
And while certifications more than doubled in that time (1,069 to 2,951), more than 17,000 certifications were still set to expire next May (as of October 2022), including certificates under both the Medical Devices Directive (MDD) and Active Implantable Medical Devices Directive, according to survey results.
Faced with such a staggering certification logjam, the European Commission in January proposed new MDR deadlines, staggering final compliance dates through 2028 based on device risk classification. The proposal also allows products marketed under the MDD to remain, under certain conditions.
Approved by the European Parliament and Council over the winter, the new deadlines extend transition timelines to May 26, 2026, for Class III custom-made implantable devices; Dec. 31, 2027, for higher-risk (mostly) Class III devices and some Class IIb implantables; and Dec. 31, 2028, for medium-risk devices, including Class II products.
“Our rules on medical devices will always prioritise patient safety and support for innovation. A combination of factors has left healthcare systems across the EU facing a risk of shortages of life-saving medical devices for patients,” EU Health and Food Safety Commissioner Stella Kyriakides said in prepared remarks. “...we propose a revised regulatory timeline to provide certainty to industry in order to continue producing essential medical devices, reducing any short-term risk of shortages, and safeguarding access for patients most in need. Member States and notified bodies should work with industry to ensure transition to the new rules provided for by the Medical Devices Regulation, without further delay.”
Sound advice, certainly, but not so sound (or realistic) of a game plan.
Clearly, the deadline extensions give medtech manufacturers and Notified Bodies more time to complete conformity assessments. But the extensions alone will not guarantee regulatory compliance because they fail to resolve the MDR’s other challenges.
Perhaps the most vexing issue that remains unsolved is the inadequate Notified Body (NB) capacity. Thirty-nine NBs currently are authorized to process MDR and IVDR (In Vitro Diagnostic Medical Device Regulation) certification requests but applicants contend that total is insufficient to handle the backlog in a timely manner. NBs, however, claim such criticism is unjustified, noting they have invested in additional staff, training, and infrastructure to manage the caseload increase.
“...notified bodies have invested extensive time and resources to expand their capacity. They have hired a considerable number of additional staff members,” the European Association of Medical Devices Notified Bodies (TEAM-NB) argued in an early August (2023) whitepaper. “Furthermore, notified bodies have actively engaged in training their existing and new personnel to ensure they possess the necessary knowledge and competence to carry out conformity assessments and certifications under the MDR. They have also enhanced their internal processes, expertise, and infrastructure to align with the new regulatory framework.”
Besides defending its capacity improvement efforts, TEAM-NB outlined a strategy in the whitepaper for further easing Notified Bodies’ workloads and expediting MDR certifications. The group suggests:
“Timely and effective coordination between all stakeholders is paramount to prevent the challenges posed by potential peaks in demand for notified body capacity around the new deadlines set by the amending regulation,” TEAM-NB concluded in its whitepaper. “Notified bodies consider the amended timelines could imply great benefits for European patients as they could ensure continued availability of essential medical devices...However, to materialize these benefits, coordinated actions of authorities, manufacturers, and notified bodies are necessary.”
Indeed, administrative coordination is crucial for MDR’s successful implementation, but it’s only one facet of the many reforms European trade groups claim is needed to prevent treatment delays amid the new rules’ transition. MedTech Europe is calling for “comprehensive” changes to the MDR and IVDR framework to ensure both current and future medical advancements reach European patients and health systems.
In an open letter to Kyriakides, MedTech Europe said the continent’s new device and diagnostics rules have not achieved their intended objectives because their structures are “unpredictable, complex, slow, and costly.”
“It is apparent there are structural issues in the regulatory framework which cannot be solved simply through its implementation,” read the Sept. 14 letter, signed by 34 national trade groups. “Reaching the objectives of the IVDR and MDR in full will require comprehensive change to improve efficiency, support innovation, and strengthen governance...”
In the letter, the trade groups propose changing the CE marking system under the MDR to make it more efficient and reduce the administrative burden. They also recommend creating an “innovation principle” that quickly connects the latest medical technologies to European patients and health systems through dedicated, fast-track assessment pathways and early dialogues with developers. The groups’ final suggestion is establishment of a single, dedicated structure to oversee the regulatory system, including NB designation and oversight.
“Only together can we deliver on the original goals of the IVDR and MDR to develop an effective and fit-for-purpose regulatory system for the benefit of European patients, health systems, and society,” the letter concluded.
Bureaucracy be damned.
Read more: bit.ly/3F3kiCP
COPD (chronic obstructive pulmonary disease) and other respiratory conditions keep him mostly confined to his home, where the air is safe to breathe. “I don’t really even come outside,” the South Memphis, Tenn., resident told WHBQ-TV (Memphis) this past spring. “I stay in the house most of the time. I worry about the pollutants in the air.”
Darwell has good reason to fret: He lives near a 45,000-square-foot sterilization plant that uses ethlyene oxide (EtO) to disinfect medical devices. The colorless, faintly sweet-smelling gas has been used for more than half a century to avert implant- and hospital-related infections, but the longstanding practice garnered new scrutiny after the U.S. Environmental Protection Agency (EPA) deemed EtO a human carcinogen in 2016.
That label has since sparked a firestorm of controversy over the gas’s long-term health hazards, pitting community activists against medtech executives in a protracted public health versus public safety tug of war. Concerns about EtO’s penchant for altering genes and changing chromosomes has consistently been met with disdain from an industry that depends on the gas to sterilize devices (pacemakers, catheters, ventilators, heart valves) ineligible for steam cleaning.
“EtO sterilization is crucial for preventing infection in patients. The process is used to sterilize half, or 20 billion, of all medical devices in the United States each year,” Khatereh Calleja, vice president of Technology and Regulatory Affairs at AdvaMed, wrote in comments to the EPA this past spring. “...it is the only effective, viable sterilization method for many medical devices. Medical device sterilization is a tiny fraction of commercial uses of EtO, representing only half of 1 percent of all commercial EtO use. But the risk of a public health threat is real if we are constrained in our ability to serve patients with the safe, effective, sterile medical technology...It is critically important that EPA recognize the importance of EtO in our healthcare system, and for individual patients.”
The EPA, however, must balance that importance with its namesake duty to protect human health and the environment. Accordingly, the agency proposed stricter new EtO emissions rules in April to help reduce lifetime cancer risks amongst commercial sterilization plant workers and host community residents. Specifically, the agency wants all 86 U.S. sterilization facilities to cut EtO emissions by 80% annually; continually monitor air pollution (and report data biannually); and reduce EtO sterilization cycle volume to a maximum 500 milligrams/liter of air. The updated standards also would require sterilization plants to conduct real-time monitoring to ensure their pollution control efforts keep indoor EtO levels below 10 parts per billion; levels above that threshold would necessitate protective equipment for workers.
“EPA’s number one priority is protecting people’s health and safety, and we are committed to taking decisive action that’s informed by the best available science,” EPA Administrator Michael S. Regan stated upon announcing the rules. “These proposals build on EPA’s outreach to communities across the nation and reflects close coordination among key federal partners. Together they would significantly reduce worker and community exposure to harmful levels of ethylene oxide.”
The EPA worked with several other agencies to draft the proposed rules, including the U.S. Food and Drug Administration (FDA), U.S. Centers for Disease Control and Prevention’s Agency for Toxic Substances and Disease Registry, and the Occupational Safety and Health Administration. The proposals are well-aligned with the Biden Administration’s Cancer Moonshot initiative and its efforts to secure environmental justice and safeguard public health in the nation’s at-risk communities (where a majority of medical sterilization plants are located).
“A lot of people feel like they put these [plants] in areas where there are mostly African Americans and people of color,” South Memphis resident Tanesha Bates declared to WHBQ, “knowing that it will cause dangerous things to happen to us.”
Dangerous and potentially deadly things: Lifetime cancer risks range from 1 in 36 to 1 in 10 for sterilization plant workers, and 1 in 25 to 1 in 12 for healthcare (hospital) sterilization operatives, EPA data indicate. An estimated 100 in 1 million people living or working near sterilization facilities—like Bates, Darwell, and breast cancer survivor Dolly M. Cross—are at risk of developing the disease, the agency claims, though the Texas Commission on Environmental Quality disputes such statistics. “EtO has not been conclusively demonstrated to cause cancer in people,” the Commission contends.
Regardless of disputed proof, the EPA is giving sterilization facilities 18 months to comply with its proposed new rules, once they are finalized (the agency is under court order to do so by March 1, 2024). Predictably, medtech industry groups are balking at the timeline and warning of “grave” supply chain consequences.
“We understand EPA’s interest in moving more quickly than usual on these priorities; however, these proposed standards are highly technical and require in-depth analyses and research on the part of organizations that utilize EtO for sterilization. They likely will require significant financial, time and resource commitments,” American Hospital Association Executive Vice President Stacey Hughes told Regan in a June 27 letter. “We are concerned that the proposed 18-month timeline is too aggressive and could result in significant disruption to the supply chain leading to decreased sterilization capacity and supply availability across the country. With device sterilization capabilities already at or near capacity across the country, we strongly encourage the agency to consider employing its traditional three-year implementation timeline to the standards if made final. This will allow these facilities more time to come into compliance prior to enforcement in an effort to help prevent the closure, temporary or permanent, of any of these facilities.”
AdvaMed supports a four-year timeline with the “ability to make case-by-case exceptions in special circumstances.” Attempting to meet the EPA’s 18-month compliance deadline could lead to the simultaneous shutdown/suspension of all U.S. sterilization facilities, the organization argues.
Thankfully, there’s an escape hatch: The FDA announced a pilot program in April to help companies adopt new ways of sterilizing approved, single-use medical devices. The voluntary program is open to in-house and contract sterilization providers that want to move a gamma radiation process to a different site; switch from gamma radiation or EtO to X-ray or electron beam radiation; or use a lower dose of gamma radiation.
Sterilization providers accepted into the program (two of the nine available slots have gone to STERIS and Andersen Sterilizers) must submit a Master File when making changes. Once the Master File is accepted into the pilot program, the pre-market approval (PMA) holder may reference the document in a post-approval report to describe the sterilization changes, thereby freeing manufacturers from submitting PMA supplements for the changes.
“FDA recognizes the need to facilitate more timely changes to alternative sterilization methods, processes, or sites among sterilization providers who use gamma radiation or EO to support sterilization supply chain resiliency,” FDA Associate Policy Commissioner Lauren K. Roth wrote in a 12-page document outlining the program. “By helping industry advance alternatives for gamma radiation and EO sterilization of medical devices, the Radiation Pilot Program seeks to help ensure patient access to safe medical devices and, through evaluation of data from pilot participants, provide insights into future regulatory approaches that may help address potential device shortages related to sterilization site, method, or process shifts, and facilitate supply chain resiliency.”
Finally, a long overdue cleaning.
Read more: bit.ly/48Sug7N
Among the more notable lines from the five-act comedy—besides the title—are “Love all, trust a few, do wrong to none...” “No legacy is so rich as honesty,” and “Good alone is good without a name, vileness is so.”
There’s another line, however, that’s far less prominent but nevertheless applicable to 21st century living: “...Oft expectation fails and most oft there; Where most it promises, and oft it hits; Where hope is coldest and despair most fits.”
Translation? Great expectations beget great disappointments.
All too true.
Consider, for example, the past year in medtech M&A. Analysts expected deal volume and value to bounce back significantly in 2023 after falling sharply last year from 2021’s exceptionally high levels.
That logic was based on the strong balance sheets diagnostics companies built from COVID-19 testing and vaccine revenue as well as “opportunistic equity and debt raises” resulting from low interest rates, MM+M (Medical Marketing and Media) reported.
“With this backdrop in mind, the conditions appear ripe for a return to historical M&A activity in 2023 and 2024 despite elevated interest rates as large-cap names in LST [life science tools] and Dx seek to deploy their cash balance or lever themselves for the appropriate asset (public or private),” predicted an SVB Securities report published earlier this year. Also contributing to SVB’s dealmaking optimism was the life sciences industry’s limited ability to raise capital and falling multiples, MM+M noted.
Great expectations.
But those falling multiples, capital-raising difficulties, and huge cash balances failed to restore medtech merger and acquisition activity to its former glory. In H1 2023, venture financing suffered its worst showing in eight years and public exits stopped altogether, pushing transaction dollars and tallies toward historic lows.
Great disappointment.
While deal volume was strong through June 30 (42 total), overall M&A value was down significantly from last year and exponentially from 2021, data from several industry sources show. Buyers poured $13.1 billion into agreements during the first six months of 2023—a paltry start compared to the previous two years’ totals ($64.8 billion in 2022, $80.5 billion in 2021).
Analysts and M&A advisors attribute this year’s leaner deal value total to the lack of megamergers—i.e., the blockbuster marriages between juggernauts like Zimmer Holdings and Biomet, Stryker Corp. and Wright Medical, DePuy Orthopaedics and Synthes Holding AG, and Orthofix and SeaSpine, among others.
“There’s not as many of the megadeals that have taken place—the larger strategics combining. There’s some of that going on, like Globus just combined with NuVasive but they were smaller companies comparatively, if you think about some of the previous years where Becton Dickinson bought out Bard and Medtronic bought out Covidien,” Dave Sheppard, managing director and COO of M&A advisory firm MedWorld Advisors, noted in a Sept. 27 webinar. “The value of deals may be less but the actual volume of deals is continuing to be very strong. They are very focused strategic deals and very opportunistic for private equity as well.”
While lingering inflation, rising interest rates, and recession fears certainly unnerved buyers this year, regulatory concerns and integration issues likely were greater obstacles to sizable acquisitions. Companies initiating megadeals will often divest parts of the business that no longer strategically fit into the combined entity’s future growth plan, M&A advisors note.
Such a strategy, of course, is not exclusive to big spenders. Small companies also divest business units to reduce operating costs and better focus on core competencies. Bioventus and Surgalign, for example, both downsized this year to tame mounting debt loads.
Bioventus sold its wound care business for $85 million to bio-implant developer LifeNet Health, maker of its TheraGenesis and TheraSkin skin substitutes. Bioventus used the $30 million in net proceeds from the May sale to help dilute its $445 million debt, part of which the company attributed to its growing operating loss from its failed CartiHeal deal, a market capitalization decline, restructuring and compensation costs, and acquisition-related expenses.
“The sale of our Wound business will enhance our liquidity,” interim Bioventus CEO Tony Bihl said in announcing the divestiture, “and enable a greater focus on execution.”
A lack of liquidity drove bankrupt Surgalign Holdings in July to sell its hardware and biologics assets to Xtant Medical Holdings and its digital health offerings to Augmedics Inc. for nearly $6 million (combined). Surgalign’s portfolio proved popular with Xtant, which purchased the financially troubled firm’s Coflex and Cofix product lines in March for $17 million. Coflex is a titanium implant placed between vertebrae to treat lumbar spinal stenosis, and Cofix is used to ease lower back pain from intervertebral disc degeneration.
Cost savings weren’t as much of a factor as reprioritized focus for Centinel Spine and Elutia Inc. The former sacrificed its global fusion business in September for total disc replacement market share, while the latter traded its orthobiologics lineup for proprietary drug-eluting biomatrix prowess.
Elutia’s $35 million divestiture price tag was typical amongst 2023 deals for lack of the larger mega-mergers that epitomized years past. There were only two transactions totaling $1 billion or more within the last 12 months—the $3.1 billion union of Globus Medical Inc. and NuVasive Inc. (February); and AMETEK’s $1.9 billion purchase of Paragon Medical (October). The year’s other “large” transactions pale by comparison: Enovis’s $847 million bid for LimaCorporate and Zimmer Biomet Holdings Inc.’s $155 million acquisition of collagen implant maker Embody Inc.
“We’ve seen some large deals,” Medword Advisors President Florence Joffroy Black explained in the webinar, “but the focus right now is on quality mid-market deals and strategic acquisitions rather than the big multi-billion-dollar deals that we’ve seen in the past.”
There were plenty of those mid-market deals and strategic acquisitions this year in orthopedics: Tyber Medical’s buyout of ADSM-Synchro Medical, Avanos Medical’s purchase of Diros Technology, Restor3d’s pickup of Conformis, Zavation Medical Products’ deal for CoreLink, Intech’s pairing with Lenkbar, Paragon Medical’s acquisition of Whitmet Inc., and ARCH Medical Solutions’ takeover of gSource LLC.
“Mid-market deals are in more demand than ever,” Joffroy-Black said. “It’s definitely the sweet spot for M&A without a doubt.”
And the path to sweeter profits, for sure.
Read more: bit.ly/3FOOIJe
Perhaps a mix of all three?
Or, possibly none of the above. Maybe it was nothing more than simple receptivity that led Cody C. Wyles, M.D., to recognize the remarkable potential of artificial intelligence (AI) within healthcare.
Maybe it was that open-mindedness that prompted Wyles—an internationally recognized hip and knee reconstruction surgeon—to verse himself in data and computer science, and form a small AI research team at the Mayo Clinic several years ago.
“It started with two or three of us meeting on nights and weekends to do proof-of-concept studies,” Wyles told a Clinic news team this past spring. “Now, we have an orthopedic artificial intelligence lab with eight surgeons, four data scientists, radiologists, and a lab manager.”
And a director—Wyles. His Orthopedic Surgery Artificial Intelligence Laboratory at Mayo Clinic is developing orthopedic surgery-focused AI solutions designed to improve both provider proficiency and patient care. Wyles has found AI to be a particularly helpful tool for radiologists, as it can effectively annotate physical features, monitor implant positioning, and predict risk from X-rays. The technology also has proven effective in processing language—Wyles’ team has used it to extract data in free-text form from typed or dictated clinical notes, and search for potential complications to patients’ cases (i.e., a draining wound).
“AI allows us to answer questions in new ways and offers insights into problems we’ve plateaued in trying to solve for many years,” noted Wyles, an assistant professor of Orthopedic Surgery and Clinical Anatomy, and senior associate consultant of Adult Hip and Knee Reconstruction at the Mayo Clinic. “It allows us to treat our patients in a more personalized way. We are new to this—our lab and its efforts have been ongoing for three years—but we have a big team and a ton of momentum. We want to lead in this space and are poised to do so with the necessary resources and infrastructure.”
Wyles’ team, however, faces fierce competition for that leadership role: AI has rapidly gained prominence in orthopedics over the last 12 months, capturing interest (and significant investment) amongst the industry’s diversified business base. Major implant manufacturers, startup software firms, and mid-size service providers are increasingly tapping the vast potential of artificial intelligence-driven technology to create powerful workflow tools for clinicians.
“We’re at the cusp of a boom of artificially intelligent orthopedic technologies,” Derek Shanahan, vice president of marketing for Denver-based digital health firm Exer, wrote in a January website post.
“With a growing tidal wave of patient data, a constant industry-wide drive to improve surgical accuracy, and higher post-surgical outcome expectations from patients, AI is sure to have a growing presence in orthopedics—both inside and outside the operating room.”
ORtelligence and Proprio helped AI expand its operating room footprint this year with their respective solutions. Seattle-based Proprio began training surgeons in late summer to use its U.S. Food and Drug Administration-cleared device that uses AI, augmented reality, and light field to help clinicians navigate spinal surgeries. The technology in its Paradigm navigation platform allows surgeons to digitally map and visualize the surgery site.
ORtelligence followed suit with the October debut of its AI-enabled software application, Rep+, which enables medtech representatives to interact remotely with surgical teams, thereby ensuring their presence during procedures. The software’s custom user interface displays all necessary tools and implants for a surgery.
AI’s presence beyond the OR grew stronger with new pre-surgical planning offerings from Formus Labs, PEEK Health S.A., and Smith+Nephew plc.
Formus Labs’ hip replacement planning software combines AI and computational biomechanics to create a surgical plan in less than an hour, while PEEK Health’s software produces live automatic surgical planning, landmark detection, and X-ray/CT scan segmentation within 30 seconds.
Smith+Nephew’s newest AI-powered surgical robotics tools include Personalized Planning and RI.INSIGHTS data visualization platform. The former works with the company’s CORI surgical system to set initial total knee implant placement based on AI-guided reference values, surgeons’ own planning preferences, and patient-specific deformities. RI.INSIGHTS, correspondingly, enables surgeons to reference individual case performance and benchmark the data against an anonymized global information bank. The platform aims to give clinicians a simple, effective way to link patient-reported outcome measures to pre-operative planning and intra-operative decisions in robotically-enabled knee replacements. Surgeon-specific dashboards allow physicians to analyze procedure data like case times, resections, and alignment, as well as ligament tensioning information from the CORI digital tensioner.
“Advanced analytics combined with the CORI Surgical System will offer a new dimension in joint arthroplasty,” Dr. Thorsten Seyler of Duke University said upon the AI tools’ release in May. “It will allow for true personalization when performing joint replacement procedures.”
Exactech and Zimmer Biomet, conversely, are leveraging AI technology to ensure personalization after joint replacement procedures. Zimmer Biomet further embedded artificial intelligence into its ZBEdge Dynamic Intelligence this past spring by integrating WalkAI into the company’s mymobility platform. WalkAI benchmarks patient gait metrics and helps surgeons predict post-hip or knee surgery gait speed. The tool also allows patients to track and measure their post-operative gait speed against their peers.
Exactech is using its beefed-up AI proficiency to improve shoulder replacement surgical outcomes. The company in early spring exclusively licensed new software from Advata that will further facilitate Predict+ integration with the firm’s Equinoxe planning app and encourage integration with other software and database. Exactech’s Predict+ uses machine learning to create personalized risk-benefit analyses for predicting shoulder replacement outcomes. The software is based on clinical experience documented in a single-shoulder prosthesis outcomes database of more than 15,000 patients.
Exactech also has hired a team of machine learning researchers and engineers to further accelerate the company’s R&D capabilities and improve its aptitude for producing AI-based software for various orthopedic applications.
Stryker Corp. is on that same accelerated pathway to AI prowess.
“I’m incredibly excited about artificial intelligence,” Stryker Chairman/CEO Kevin Lobo told Fox Business Network’s “Claman Countdown” in February. “[Stryker AI] is now looking at how else we can deploy AI across the depth of our portfolios. We already had one application for shoulder replacement, where we used AI based on a scan to actually suggest to the surgeon what type of implant they should use...So this is the future. There’s no question AI will be proliferated across all of Stryker.”
And all of orthopedics, according to ChatGPT:
In the world of orthopaedics, AI takes flight, bringing benefits that shine so bright. With precision and insight, it aids the way, enhancing patient care day by day...In orthopaedics, AI takes its stance, improve lives with its intelligent dance. A partner to experts, a valuable ally, embracing the future, where innovation will fly.1
Not bad for a first-time AI poet.
Reference
Read more: bit.ly/3FKg5nF
Forty months after declaring the SARS-CoV-2 virus a global threat, WHO’s director-general officially ended the COVID-19 public health emergency on May 11. “For more than a year, the pandemic has been on a downward trend…” Tedros Adhanom Ghebreyesus stated at a media briefing in Geneva. “This trend has allowed most countries to return to life as we knew it before COVID-19. It is therefore with great hope that I declare COVID-19 over as a global health emergency.”
Free at last.
Free with a caveat, actually: Although the global health emergency is over, the pandemic itself is still public threat, Adhanom Ghebreyesus warned, virulent enough to claim a life every three minutes and savvy enough to evade extinction via perpetual mutations.
So the pandemic continues. And, as history has repeatedly proven, it probably will continue for quite some time. Pandemics seldom have clean conclusions; their endings tend to be ragged and messy—similar to life itself. Some return repeatedly before fading (the Black Death reappeared more than 40 times over 400 years), while others never completely go away.
COVID-19 will likely become one of those everlasting nuisances, lurking in the shadows to disrupt life every once in a while. The world now has to adjust to its new normal.
It won’t be easy. “As we have seen time and time again throughout human history,” a Time commentary reminded readers, “pandemics do not end—they echo.”
Better get used to the reverberation.
MDR’s Maddening Merry-Go-Round
Keep Cool About the Rule.That is the advice Helena Holma is offering to startups and rookie entrepreneurs intimidated by the new Medical Device Regulation (MDR). “If you are a startup within healthtech—embrace the regulations,” Holma wrote in an early January blog. “There is no way around them and even if they may seem discouraging, remember they are for a good cause—to ensure patient safety and privacy. If you are well familiar with the regulations and include them in your business strategy, it will give you a competitive advantage.”
Perhaps, but MDR compliance is actually more of a necessity these days as Europe transitions to its long-awaited, much-debated, widely-hated medical device certification rules. Implemented in May 2017, European lawmakers drafted the MDR to update the continent’s archaic Medical Device Directive and harmonize the regulatory review and product approval process across all EU member states.
Although the medtech industry lauded the modernized rules—hopeful they would foster more patient-oriented innovation and better support the specific needs of small and medium-sized enterprises—manufacturers took issue with the MDR’s final compliance deadline, contending the three-year window was “unrealistic” and would lead to widespread device shortages. Calls for a deadline extension intensified as the May 26, 2020, due date approached, though the industry received an unexpected (but nevertheless welcome) one-year reprieve courtesy of COVID-19.
Since then, a growing chorus of industry groups and medtech firms have clamored for an extension to the MDR’s May 26, 2024, re-certification deadline, citing massive Notified Body backlogs and protracted reauthorization waits. As of March (2023), those waits averaged anywhere from six to 23 months (for QMS+product certification applications), while authorization requests nearly doubled, going from 6,188 in April 2022 to 11,418 in March 2023, European Commission survey data indicate.
And while certifications more than doubled in that time (1,069 to 2,951), more than 17,000 certifications were still set to expire next May (as of October 2022), including certificates under both the Medical Devices Directive (MDD) and Active Implantable Medical Devices Directive, according to survey results.
Faced with such a staggering certification logjam, the European Commission in January proposed new MDR deadlines, staggering final compliance dates through 2028 based on device risk classification. The proposal also allows products marketed under the MDD to remain, under certain conditions.
Approved by the European Parliament and Council over the winter, the new deadlines extend transition timelines to May 26, 2026, for Class III custom-made implantable devices; Dec. 31, 2027, for higher-risk (mostly) Class III devices and some Class IIb implantables; and Dec. 31, 2028, for medium-risk devices, including Class II products.
“Our rules on medical devices will always prioritise patient safety and support for innovation. A combination of factors has left healthcare systems across the EU facing a risk of shortages of life-saving medical devices for patients,” EU Health and Food Safety Commissioner Stella Kyriakides said in prepared remarks. “...we propose a revised regulatory timeline to provide certainty to industry in order to continue producing essential medical devices, reducing any short-term risk of shortages, and safeguarding access for patients most in need. Member States and notified bodies should work with industry to ensure transition to the new rules provided for by the Medical Devices Regulation, without further delay.”
Sound advice, certainly, but not so sound (or realistic) of a game plan.
Clearly, the deadline extensions give medtech manufacturers and Notified Bodies more time to complete conformity assessments. But the extensions alone will not guarantee regulatory compliance because they fail to resolve the MDR’s other challenges.
Perhaps the most vexing issue that remains unsolved is the inadequate Notified Body (NB) capacity. Thirty-nine NBs currently are authorized to process MDR and IVDR (In Vitro Diagnostic Medical Device Regulation) certification requests but applicants contend that total is insufficient to handle the backlog in a timely manner. NBs, however, claim such criticism is unjustified, noting they have invested in additional staff, training, and infrastructure to manage the caseload increase.
“...notified bodies have invested extensive time and resources to expand their capacity. They have hired a considerable number of additional staff members,” the European Association of Medical Devices Notified Bodies (TEAM-NB) argued in an early August (2023) whitepaper. “Furthermore, notified bodies have actively engaged in training their existing and new personnel to ensure they possess the necessary knowledge and competence to carry out conformity assessments and certifications under the MDR. They have also enhanced their internal processes, expertise, and infrastructure to align with the new regulatory framework.”
Besides defending its capacity improvement efforts, TEAM-NB outlined a strategy in the whitepaper for further easing Notified Bodies’ workloads and expediting MDR certifications. The group suggests:
- Making better use of hybrid audits, and combining audits under the directives and regulations for legacy products;
- Abandoning technical documentation sampling for MDR devices;
- Promptly adding designation codes to NBs;
- Improving dialogue between regulators and stakeholders;
- Reducing NB designation timelines;
- Developing alternative competency demonstration methods;
- Harmonizing procedures and enhancing predictability; and
- Increasing complete (and timely) MDR applications.
“Timely and effective coordination between all stakeholders is paramount to prevent the challenges posed by potential peaks in demand for notified body capacity around the new deadlines set by the amending regulation,” TEAM-NB concluded in its whitepaper. “Notified bodies consider the amended timelines could imply great benefits for European patients as they could ensure continued availability of essential medical devices...However, to materialize these benefits, coordinated actions of authorities, manufacturers, and notified bodies are necessary.”
Indeed, administrative coordination is crucial for MDR’s successful implementation, but it’s only one facet of the many reforms European trade groups claim is needed to prevent treatment delays amid the new rules’ transition. MedTech Europe is calling for “comprehensive” changes to the MDR and IVDR framework to ensure both current and future medical advancements reach European patients and health systems.
In an open letter to Kyriakides, MedTech Europe said the continent’s new device and diagnostics rules have not achieved their intended objectives because their structures are “unpredictable, complex, slow, and costly.”
“It is apparent there are structural issues in the regulatory framework which cannot be solved simply through its implementation,” read the Sept. 14 letter, signed by 34 national trade groups. “Reaching the objectives of the IVDR and MDR in full will require comprehensive change to improve efficiency, support innovation, and strengthen governance...”
In the letter, the trade groups propose changing the CE marking system under the MDR to make it more efficient and reduce the administrative burden. They also recommend creating an “innovation principle” that quickly connects the latest medical technologies to European patients and health systems through dedicated, fast-track assessment pathways and early dialogues with developers. The groups’ final suggestion is establishment of a single, dedicated structure to oversee the regulatory system, including NB designation and oversight.
“Only together can we deliver on the original goals of the IVDR and MDR to develop an effective and fit-for-purpose regulatory system for the benefit of European patients, health systems, and society,” the letter concluded.
Bureaucracy be damned.
Read more: bit.ly/3F3kiCP
A Clean Start?
Darwell doesn’t venture out much these days.COPD (chronic obstructive pulmonary disease) and other respiratory conditions keep him mostly confined to his home, where the air is safe to breathe. “I don’t really even come outside,” the South Memphis, Tenn., resident told WHBQ-TV (Memphis) this past spring. “I stay in the house most of the time. I worry about the pollutants in the air.”
Darwell has good reason to fret: He lives near a 45,000-square-foot sterilization plant that uses ethlyene oxide (EtO) to disinfect medical devices. The colorless, faintly sweet-smelling gas has been used for more than half a century to avert implant- and hospital-related infections, but the longstanding practice garnered new scrutiny after the U.S. Environmental Protection Agency (EPA) deemed EtO a human carcinogen in 2016.
That label has since sparked a firestorm of controversy over the gas’s long-term health hazards, pitting community activists against medtech executives in a protracted public health versus public safety tug of war. Concerns about EtO’s penchant for altering genes and changing chromosomes has consistently been met with disdain from an industry that depends on the gas to sterilize devices (pacemakers, catheters, ventilators, heart valves) ineligible for steam cleaning.
“EtO sterilization is crucial for preventing infection in patients. The process is used to sterilize half, or 20 billion, of all medical devices in the United States each year,” Khatereh Calleja, vice president of Technology and Regulatory Affairs at AdvaMed, wrote in comments to the EPA this past spring. “...it is the only effective, viable sterilization method for many medical devices. Medical device sterilization is a tiny fraction of commercial uses of EtO, representing only half of 1 percent of all commercial EtO use. But the risk of a public health threat is real if we are constrained in our ability to serve patients with the safe, effective, sterile medical technology...It is critically important that EPA recognize the importance of EtO in our healthcare system, and for individual patients.”
The EPA, however, must balance that importance with its namesake duty to protect human health and the environment. Accordingly, the agency proposed stricter new EtO emissions rules in April to help reduce lifetime cancer risks amongst commercial sterilization plant workers and host community residents. Specifically, the agency wants all 86 U.S. sterilization facilities to cut EtO emissions by 80% annually; continually monitor air pollution (and report data biannually); and reduce EtO sterilization cycle volume to a maximum 500 milligrams/liter of air. The updated standards also would require sterilization plants to conduct real-time monitoring to ensure their pollution control efforts keep indoor EtO levels below 10 parts per billion; levels above that threshold would necessitate protective equipment for workers.
“EPA’s number one priority is protecting people’s health and safety, and we are committed to taking decisive action that’s informed by the best available science,” EPA Administrator Michael S. Regan stated upon announcing the rules. “These proposals build on EPA’s outreach to communities across the nation and reflects close coordination among key federal partners. Together they would significantly reduce worker and community exposure to harmful levels of ethylene oxide.”
The EPA worked with several other agencies to draft the proposed rules, including the U.S. Food and Drug Administration (FDA), U.S. Centers for Disease Control and Prevention’s Agency for Toxic Substances and Disease Registry, and the Occupational Safety and Health Administration. The proposals are well-aligned with the Biden Administration’s Cancer Moonshot initiative and its efforts to secure environmental justice and safeguard public health in the nation’s at-risk communities (where a majority of medical sterilization plants are located).
“A lot of people feel like they put these [plants] in areas where there are mostly African Americans and people of color,” South Memphis resident Tanesha Bates declared to WHBQ, “knowing that it will cause dangerous things to happen to us.”
Dangerous and potentially deadly things: Lifetime cancer risks range from 1 in 36 to 1 in 10 for sterilization plant workers, and 1 in 25 to 1 in 12 for healthcare (hospital) sterilization operatives, EPA data indicate. An estimated 100 in 1 million people living or working near sterilization facilities—like Bates, Darwell, and breast cancer survivor Dolly M. Cross—are at risk of developing the disease, the agency claims, though the Texas Commission on Environmental Quality disputes such statistics. “EtO has not been conclusively demonstrated to cause cancer in people,” the Commission contends.
Regardless of disputed proof, the EPA is giving sterilization facilities 18 months to comply with its proposed new rules, once they are finalized (the agency is under court order to do so by March 1, 2024). Predictably, medtech industry groups are balking at the timeline and warning of “grave” supply chain consequences.
“We understand EPA’s interest in moving more quickly than usual on these priorities; however, these proposed standards are highly technical and require in-depth analyses and research on the part of organizations that utilize EtO for sterilization. They likely will require significant financial, time and resource commitments,” American Hospital Association Executive Vice President Stacey Hughes told Regan in a June 27 letter. “We are concerned that the proposed 18-month timeline is too aggressive and could result in significant disruption to the supply chain leading to decreased sterilization capacity and supply availability across the country. With device sterilization capabilities already at or near capacity across the country, we strongly encourage the agency to consider employing its traditional three-year implementation timeline to the standards if made final. This will allow these facilities more time to come into compliance prior to enforcement in an effort to help prevent the closure, temporary or permanent, of any of these facilities.”
AdvaMed supports a four-year timeline with the “ability to make case-by-case exceptions in special circumstances.” Attempting to meet the EPA’s 18-month compliance deadline could lead to the simultaneous shutdown/suspension of all U.S. sterilization facilities, the organization argues.
Thankfully, there’s an escape hatch: The FDA announced a pilot program in April to help companies adopt new ways of sterilizing approved, single-use medical devices. The voluntary program is open to in-house and contract sterilization providers that want to move a gamma radiation process to a different site; switch from gamma radiation or EtO to X-ray or electron beam radiation; or use a lower dose of gamma radiation.
Sterilization providers accepted into the program (two of the nine available slots have gone to STERIS and Andersen Sterilizers) must submit a Master File when making changes. Once the Master File is accepted into the pilot program, the pre-market approval (PMA) holder may reference the document in a post-approval report to describe the sterilization changes, thereby freeing manufacturers from submitting PMA supplements for the changes.
“FDA recognizes the need to facilitate more timely changes to alternative sterilization methods, processes, or sites among sterilization providers who use gamma radiation or EO to support sterilization supply chain resiliency,” FDA Associate Policy Commissioner Lauren K. Roth wrote in a 12-page document outlining the program. “By helping industry advance alternatives for gamma radiation and EO sterilization of medical devices, the Radiation Pilot Program seeks to help ensure patient access to safe medical devices and, through evaluation of data from pilot participants, provide insights into future regulatory approaches that may help address potential device shortages related to sterilization site, method, or process shifts, and facilitate supply chain resiliency.”
Finally, a long overdue cleaning.
Read more: bit.ly/48Sug7N
Mega-M&A MIA
It may not be the most favored or famous Shakespeare play (reputedly unpopular even in the Bard’s day), but “All’s Well That Ends Well” certainly is rife with familiar quotes.Among the more notable lines from the five-act comedy—besides the title—are “Love all, trust a few, do wrong to none...” “No legacy is so rich as honesty,” and “Good alone is good without a name, vileness is so.”
There’s another line, however, that’s far less prominent but nevertheless applicable to 21st century living: “...Oft expectation fails and most oft there; Where most it promises, and oft it hits; Where hope is coldest and despair most fits.”
Translation? Great expectations beget great disappointments.
All too true.
Consider, for example, the past year in medtech M&A. Analysts expected deal volume and value to bounce back significantly in 2023 after falling sharply last year from 2021’s exceptionally high levels.
That logic was based on the strong balance sheets diagnostics companies built from COVID-19 testing and vaccine revenue as well as “opportunistic equity and debt raises” resulting from low interest rates, MM+M (Medical Marketing and Media) reported.
“With this backdrop in mind, the conditions appear ripe for a return to historical M&A activity in 2023 and 2024 despite elevated interest rates as large-cap names in LST [life science tools] and Dx seek to deploy their cash balance or lever themselves for the appropriate asset (public or private),” predicted an SVB Securities report published earlier this year. Also contributing to SVB’s dealmaking optimism was the life sciences industry’s limited ability to raise capital and falling multiples, MM+M noted.
Great expectations.
But those falling multiples, capital-raising difficulties, and huge cash balances failed to restore medtech merger and acquisition activity to its former glory. In H1 2023, venture financing suffered its worst showing in eight years and public exits stopped altogether, pushing transaction dollars and tallies toward historic lows.
Great disappointment.
While deal volume was strong through June 30 (42 total), overall M&A value was down significantly from last year and exponentially from 2021, data from several industry sources show. Buyers poured $13.1 billion into agreements during the first six months of 2023—a paltry start compared to the previous two years’ totals ($64.8 billion in 2022, $80.5 billion in 2021).
Analysts and M&A advisors attribute this year’s leaner deal value total to the lack of megamergers—i.e., the blockbuster marriages between juggernauts like Zimmer Holdings and Biomet, Stryker Corp. and Wright Medical, DePuy Orthopaedics and Synthes Holding AG, and Orthofix and SeaSpine, among others.
“There’s not as many of the megadeals that have taken place—the larger strategics combining. There’s some of that going on, like Globus just combined with NuVasive but they were smaller companies comparatively, if you think about some of the previous years where Becton Dickinson bought out Bard and Medtronic bought out Covidien,” Dave Sheppard, managing director and COO of M&A advisory firm MedWorld Advisors, noted in a Sept. 27 webinar. “The value of deals may be less but the actual volume of deals is continuing to be very strong. They are very focused strategic deals and very opportunistic for private equity as well.”
While lingering inflation, rising interest rates, and recession fears certainly unnerved buyers this year, regulatory concerns and integration issues likely were greater obstacles to sizable acquisitions. Companies initiating megadeals will often divest parts of the business that no longer strategically fit into the combined entity’s future growth plan, M&A advisors note.
Such a strategy, of course, is not exclusive to big spenders. Small companies also divest business units to reduce operating costs and better focus on core competencies. Bioventus and Surgalign, for example, both downsized this year to tame mounting debt loads.
Bioventus sold its wound care business for $85 million to bio-implant developer LifeNet Health, maker of its TheraGenesis and TheraSkin skin substitutes. Bioventus used the $30 million in net proceeds from the May sale to help dilute its $445 million debt, part of which the company attributed to its growing operating loss from its failed CartiHeal deal, a market capitalization decline, restructuring and compensation costs, and acquisition-related expenses.
“The sale of our Wound business will enhance our liquidity,” interim Bioventus CEO Tony Bihl said in announcing the divestiture, “and enable a greater focus on execution.”
A lack of liquidity drove bankrupt Surgalign Holdings in July to sell its hardware and biologics assets to Xtant Medical Holdings and its digital health offerings to Augmedics Inc. for nearly $6 million (combined). Surgalign’s portfolio proved popular with Xtant, which purchased the financially troubled firm’s Coflex and Cofix product lines in March for $17 million. Coflex is a titanium implant placed between vertebrae to treat lumbar spinal stenosis, and Cofix is used to ease lower back pain from intervertebral disc degeneration.
Cost savings weren’t as much of a factor as reprioritized focus for Centinel Spine and Elutia Inc. The former sacrificed its global fusion business in September for total disc replacement market share, while the latter traded its orthobiologics lineup for proprietary drug-eluting biomatrix prowess.
Elutia’s $35 million divestiture price tag was typical amongst 2023 deals for lack of the larger mega-mergers that epitomized years past. There were only two transactions totaling $1 billion or more within the last 12 months—the $3.1 billion union of Globus Medical Inc. and NuVasive Inc. (February); and AMETEK’s $1.9 billion purchase of Paragon Medical (October). The year’s other “large” transactions pale by comparison: Enovis’s $847 million bid for LimaCorporate and Zimmer Biomet Holdings Inc.’s $155 million acquisition of collagen implant maker Embody Inc.
“We’ve seen some large deals,” Medword Advisors President Florence Joffroy Black explained in the webinar, “but the focus right now is on quality mid-market deals and strategic acquisitions rather than the big multi-billion-dollar deals that we’ve seen in the past.”
There were plenty of those mid-market deals and strategic acquisitions this year in orthopedics: Tyber Medical’s buyout of ADSM-Synchro Medical, Avanos Medical’s purchase of Diros Technology, Restor3d’s pickup of Conformis, Zavation Medical Products’ deal for CoreLink, Intech’s pairing with Lenkbar, Paragon Medical’s acquisition of Whitmet Inc., and ARCH Medical Solutions’ takeover of gSource LLC.
“Mid-market deals are in more demand than ever,” Joffroy-Black said. “It’s definitely the sweet spot for M&A without a doubt.”
And the path to sweeter profits, for sure.
Read more: bit.ly/3FOOIJe
Artificially Intelligent Orthopedics
Was it a hunch? Insight? Incredible perspicacity?Perhaps a mix of all three?
Or, possibly none of the above. Maybe it was nothing more than simple receptivity that led Cody C. Wyles, M.D., to recognize the remarkable potential of artificial intelligence (AI) within healthcare.
Maybe it was that open-mindedness that prompted Wyles—an internationally recognized hip and knee reconstruction surgeon—to verse himself in data and computer science, and form a small AI research team at the Mayo Clinic several years ago.
“It started with two or three of us meeting on nights and weekends to do proof-of-concept studies,” Wyles told a Clinic news team this past spring. “Now, we have an orthopedic artificial intelligence lab with eight surgeons, four data scientists, radiologists, and a lab manager.”
And a director—Wyles. His Orthopedic Surgery Artificial Intelligence Laboratory at Mayo Clinic is developing orthopedic surgery-focused AI solutions designed to improve both provider proficiency and patient care. Wyles has found AI to be a particularly helpful tool for radiologists, as it can effectively annotate physical features, monitor implant positioning, and predict risk from X-rays. The technology also has proven effective in processing language—Wyles’ team has used it to extract data in free-text form from typed or dictated clinical notes, and search for potential complications to patients’ cases (i.e., a draining wound).
“AI allows us to answer questions in new ways and offers insights into problems we’ve plateaued in trying to solve for many years,” noted Wyles, an assistant professor of Orthopedic Surgery and Clinical Anatomy, and senior associate consultant of Adult Hip and Knee Reconstruction at the Mayo Clinic. “It allows us to treat our patients in a more personalized way. We are new to this—our lab and its efforts have been ongoing for three years—but we have a big team and a ton of momentum. We want to lead in this space and are poised to do so with the necessary resources and infrastructure.”
Wyles’ team, however, faces fierce competition for that leadership role: AI has rapidly gained prominence in orthopedics over the last 12 months, capturing interest (and significant investment) amongst the industry’s diversified business base. Major implant manufacturers, startup software firms, and mid-size service providers are increasingly tapping the vast potential of artificial intelligence-driven technology to create powerful workflow tools for clinicians.
“We’re at the cusp of a boom of artificially intelligent orthopedic technologies,” Derek Shanahan, vice president of marketing for Denver-based digital health firm Exer, wrote in a January website post.
“With a growing tidal wave of patient data, a constant industry-wide drive to improve surgical accuracy, and higher post-surgical outcome expectations from patients, AI is sure to have a growing presence in orthopedics—both inside and outside the operating room.”
ORtelligence and Proprio helped AI expand its operating room footprint this year with their respective solutions. Seattle-based Proprio began training surgeons in late summer to use its U.S. Food and Drug Administration-cleared device that uses AI, augmented reality, and light field to help clinicians navigate spinal surgeries. The technology in its Paradigm navigation platform allows surgeons to digitally map and visualize the surgery site.
ORtelligence followed suit with the October debut of its AI-enabled software application, Rep+, which enables medtech representatives to interact remotely with surgical teams, thereby ensuring their presence during procedures. The software’s custom user interface displays all necessary tools and implants for a surgery.
AI’s presence beyond the OR grew stronger with new pre-surgical planning offerings from Formus Labs, PEEK Health S.A., and Smith+Nephew plc.
Formus Labs’ hip replacement planning software combines AI and computational biomechanics to create a surgical plan in less than an hour, while PEEK Health’s software produces live automatic surgical planning, landmark detection, and X-ray/CT scan segmentation within 30 seconds.
Smith+Nephew’s newest AI-powered surgical robotics tools include Personalized Planning and RI.INSIGHTS data visualization platform. The former works with the company’s CORI surgical system to set initial total knee implant placement based on AI-guided reference values, surgeons’ own planning preferences, and patient-specific deformities. RI.INSIGHTS, correspondingly, enables surgeons to reference individual case performance and benchmark the data against an anonymized global information bank. The platform aims to give clinicians a simple, effective way to link patient-reported outcome measures to pre-operative planning and intra-operative decisions in robotically-enabled knee replacements. Surgeon-specific dashboards allow physicians to analyze procedure data like case times, resections, and alignment, as well as ligament tensioning information from the CORI digital tensioner.
“Advanced analytics combined with the CORI Surgical System will offer a new dimension in joint arthroplasty,” Dr. Thorsten Seyler of Duke University said upon the AI tools’ release in May. “It will allow for true personalization when performing joint replacement procedures.”
Exactech and Zimmer Biomet, conversely, are leveraging AI technology to ensure personalization after joint replacement procedures. Zimmer Biomet further embedded artificial intelligence into its ZBEdge Dynamic Intelligence this past spring by integrating WalkAI into the company’s mymobility platform. WalkAI benchmarks patient gait metrics and helps surgeons predict post-hip or knee surgery gait speed. The tool also allows patients to track and measure their post-operative gait speed against their peers.
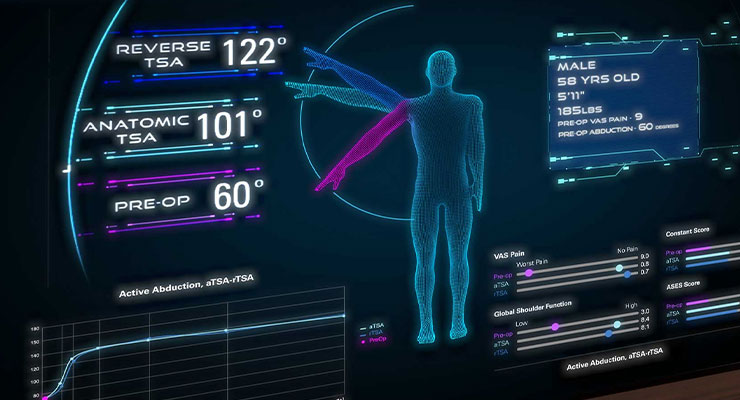
Exactech is using its beefed-up AI proficiency to improve shoulder replacement surgical outcomes. The company in early spring exclusively licensed new software from Advata that will further facilitate Predict+ integration with the firm’s Equinoxe planning app and encourage integration with other software and database. Exactech’s Predict+ uses machine learning to create personalized risk-benefit analyses for predicting shoulder replacement outcomes. The software is based on clinical experience documented in a single-shoulder prosthesis outcomes database of more than 15,000 patients.
Exactech also has hired a team of machine learning researchers and engineers to further accelerate the company’s R&D capabilities and improve its aptitude for producing AI-based software for various orthopedic applications.
Stryker Corp. is on that same accelerated pathway to AI prowess.
“I’m incredibly excited about artificial intelligence,” Stryker Chairman/CEO Kevin Lobo told Fox Business Network’s “Claman Countdown” in February. “[Stryker AI] is now looking at how else we can deploy AI across the depth of our portfolios. We already had one application for shoulder replacement, where we used AI based on a scan to actually suggest to the surgeon what type of implant they should use...So this is the future. There’s no question AI will be proliferated across all of Stryker.”
And all of orthopedics, according to ChatGPT:
In the world of orthopaedics, AI takes flight, bringing benefits that shine so bright. With precision and insight, it aids the way, enhancing patient care day by day...In orthopaedics, AI takes its stance, improve lives with its intelligent dance. A partner to experts, a valuable ally, embracing the future, where innovation will fly.1
Not bad for a first-time AI poet.
Reference
Read more: bit.ly/3FKg5nF
