Sean Fenske, Editor01.12.17
While the discussion of personalized healthcare is prevalent with regard to implants, chronic disease, and pharmaceuticals, it is rarely considered for diagnostic imaging. Instead, a single type of technology can be used for a variety of applications without it truly being an ideal fit.
With this in mind, Esaote has developed a flexible solution that enables a patient to be imaged in both the supine and weight-bearing positions in about 10 minutes. Further, the system is at a size that enables it to be used in a doctor’s office rather than being limited to a hospital.
While attending NASS (North American Spine Society) in 2016, I visited with Esaote and got a look at their newest MRI offering. I also had a conversation with Wim van Kemenade, MRI communication and sales support for the company. He provided insights on the G-Scan Brio, the company’s thinking behind the device, and what’s ahead in the imaging sector.
Sean Fenske: Can you briefly give a little background on Esaote?
Wim van Kemenade: Esaote was founded in 1982 as a startup, spun-off of a large Italian industry group. Today, Esaote has about 1,300 employees, sales of €280 million, and offices in all major countries.
Regarding MRI, Esaote, like all other companies, started developing and selling whole body MRI in the eighties. In the early nineties, Esaote decided to focus on dedicated MSK MRI systems with the first dedicated MRI on display at the RSNA meeting of 1994. Starting with a small, limbs-only scanner, the company now has a product offering that covers a complete range of MSK MRI applications, including weight-bearing MRI.
Important to mention is the introduction of the eXP imaging platform in 2013. The eXP platform (HW and SW) was a real quantum leap in image quality and acquisition speed, introducing sophisticated 3D Steady State sequences (e.g., for high resolution cartilage imaging and patented high-speed acquisition algorithms).
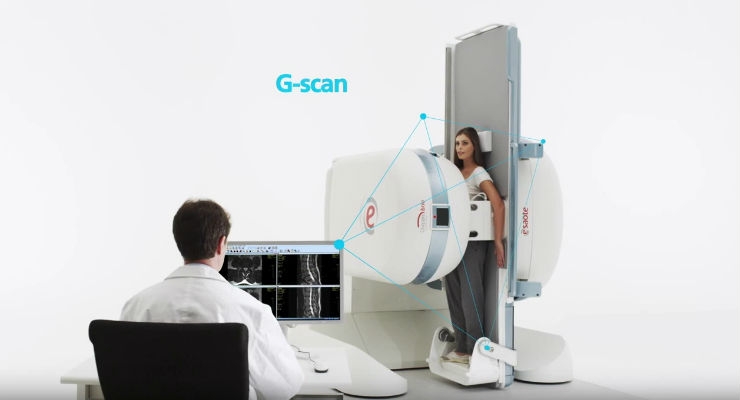
Fenske: Esaote’s latest imaging solution is the G-Scan Brio. What makes this a unique technology in the industry?
van Kemenade: The G-scan offers both high quality, general MSK MRI imaging as weight-bearing (WB) MRI in a compact format. The G-Scan MRI can be installed in only 25 m2 or 2,500 sq. ft. and runs off a standard 110/220 V outlet. Running costs are extremely low so with G-Scan, WB MRI becomes available for virtually any setting, whether clinic, hospital, or university.
Fenske: Why is it important to visualize a herniated disc in both standing and supine positions?
van Kemenade: As you can imagine, pathologies like herniation are subject to biomechanical changes due to the changed curvature of the spine under load (sitting or standing versus lying down). Being able to visualize these changes is important for the spine surgeon to choose the best therapeutic approach. Studies indicate that in 20 to 30 percent of the cases, there are significant changes between erect and recumbent MRI.
Supine MRI remains the technique of choice for detecting degenerative disc disease associated with acute and chronic low back pain. However, in about one of three cases, conventional MRI performed in the supine position is unable to answer the clinical question. In these cases, or if it is necessary to assess the degree of spinal instability more accurately (particularly if surgical therapy is scheduled), the dedicated equipment for performing an upright MRI can be a complementary investigation to a traditional MRI survey.
Fenske: Before the G-Scan made this a sort of “one-step imaging process,” how was this comparison done in the past?
van Kemenade: The only method to visualize the WB effect was with x-ray, which gives little soft-tissue information such as the bulging of a disk or the impingement of nerve roots caused by the rotation of the disk. According to spine surgeons we spoke with, MRI in the weight-bearing position is the only logical step to conduct as it gives important feedback on the soft tissue that cannot be obtained by other modalities.
Fenske: What were the most notable challenges in the development of this system and how did you overcome them?
van Kemenade: WB-MRI poses two important challenges—movement and artifacts. Patients who have severe back pain often cannot stand for a long period of time. Thanks to the eXP platform (speed plus image quality) and the clinical feedback from two important reference sites (Sports Klinik Stuttgart, Germany and Parker Institute, Copenhagen, Denmark), we were able to develop a “10-minute weight-bearing imaging protocol” to comply with these requisites.
In short, we position the patient at about 85 degrees, which, from a biomechanical point, gives an almost full WB effect, but at the same time, stabilizes the patient so there is less movement. As the main target is biomechanics, a high-res, isotropic 3D scan of the spine is first performed and then followed by a T2 weighted scan—all in about 10 minutes.
The 3D gives the possibility to perform subsequent reconstruction in any desired plane to evaluate biomechanics and the T2 is pathology oriented. After this, the patient table is rotated and the exam is completed with “normal” or standard imaging protocol.
Fenske: Will you look to adapt the technology for other imaging applications? Do you have any specific targets in mind?
van Kemenade: For the WB-MRI application, there is an interest for specific pathologies of the female pelvis where WB MRI could give an added diagnostic value. We have some sites that are looking into this; the first results are very promising. We are also experimenting with real-time MRI or MRI fluoroscopy as our system and coil design has taken this application into consideration from the beginning. Also hearing initial positive feedback in particular from sites specialized in sports medicine.
Fenske: What has been the industry response to this technology?
van Kemenade: Regarding the industry, there will always be a place for smaller companies that address particular clinical needs. Large companies work in a different economical framework; they have to sell large quantities to make it economically interesting for them. Just think of the costs of product introductions (marketing, training, roadshows, etc.) in a large, worldwide organization. For a company the size of Esaote, we are big enough to sustain the MRI R&D costs but small enough to be profitable with smaller sales numbers. MSK MRI is a very big chunk of the total MRI workload and, next to the particular WB-MRI application, we simply offer systems that can do excellent MSK-MRI imaging with a cost/benefit ratio that is clearly better than traditional MRI.
Fenske: Where is the imaging industry headed? What do you foresee coming down the pipeline five to ten years out?
van Kemenade: My personal vision is that, little by little, MRI will head into the x-ray direction where there are different systems for different needs, from a simple C-arm to sophisticated bi-plane angio/cardio systems. No doctor will consider examining a broken wrist on a bi-plane cardio x-ray. Even if this was possible, this would be a clear waste of money and resources. Now, why is the same principle not applied in MRI? Clinical papers show that, for example, the diagnostic outcome for meniscal tear using a 1.5T and a dedicated system are the same. In the medical world, changing the mindset is a slow process but the cost constraints in medical imaging are clearly in our favor and will speed-up this process.
Fenske: Any other comments or thoughts you’d like to share?
van Kemenade: Over the last few years, dedicated MRI has definitely evolved, with a huge improvement in image quality and reduced scan times. Unfortunately, many radiologists still have the images they saw maybe five years ago in mind. Today, every time we show current images (DICOM) at congresses like RSNA or ECR, we always get feedback like, “I didn’t expect such good quality,” or “Are these made with your small systems?” Unfortunately, it takes time to get this message into the market. From this point of view, it would, of course, be nice to have the big marketing budget of a large multi-national.
Get a look at the G-Scan Brio.
With this in mind, Esaote has developed a flexible solution that enables a patient to be imaged in both the supine and weight-bearing positions in about 10 minutes. Further, the system is at a size that enables it to be used in a doctor’s office rather than being limited to a hospital.
While attending NASS (North American Spine Society) in 2016, I visited with Esaote and got a look at their newest MRI offering. I also had a conversation with Wim van Kemenade, MRI communication and sales support for the company. He provided insights on the G-Scan Brio, the company’s thinking behind the device, and what’s ahead in the imaging sector.
Sean Fenske: Can you briefly give a little background on Esaote?
Wim van Kemenade: Esaote was founded in 1982 as a startup, spun-off of a large Italian industry group. Today, Esaote has about 1,300 employees, sales of €280 million, and offices in all major countries.
Regarding MRI, Esaote, like all other companies, started developing and selling whole body MRI in the eighties. In the early nineties, Esaote decided to focus on dedicated MSK MRI systems with the first dedicated MRI on display at the RSNA meeting of 1994. Starting with a small, limbs-only scanner, the company now has a product offering that covers a complete range of MSK MRI applications, including weight-bearing MRI.
Important to mention is the introduction of the eXP imaging platform in 2013. The eXP platform (HW and SW) was a real quantum leap in image quality and acquisition speed, introducing sophisticated 3D Steady State sequences (e.g., for high resolution cartilage imaging and patented high-speed acquisition algorithms).
Fenske: Esaote’s latest imaging solution is the G-Scan Brio. What makes this a unique technology in the industry?
van Kemenade: The G-scan offers both high quality, general MSK MRI imaging as weight-bearing (WB) MRI in a compact format. The G-Scan MRI can be installed in only 25 m2 or 2,500 sq. ft. and runs off a standard 110/220 V outlet. Running costs are extremely low so with G-Scan, WB MRI becomes available for virtually any setting, whether clinic, hospital, or university.
Fenske: Why is it important to visualize a herniated disc in both standing and supine positions?
van Kemenade: As you can imagine, pathologies like herniation are subject to biomechanical changes due to the changed curvature of the spine under load (sitting or standing versus lying down). Being able to visualize these changes is important for the spine surgeon to choose the best therapeutic approach. Studies indicate that in 20 to 30 percent of the cases, there are significant changes between erect and recumbent MRI.
Supine MRI remains the technique of choice for detecting degenerative disc disease associated with acute and chronic low back pain. However, in about one of three cases, conventional MRI performed in the supine position is unable to answer the clinical question. In these cases, or if it is necessary to assess the degree of spinal instability more accurately (particularly if surgical therapy is scheduled), the dedicated equipment for performing an upright MRI can be a complementary investigation to a traditional MRI survey.
Fenske: Before the G-Scan made this a sort of “one-step imaging process,” how was this comparison done in the past?
van Kemenade: The only method to visualize the WB effect was with x-ray, which gives little soft-tissue information such as the bulging of a disk or the impingement of nerve roots caused by the rotation of the disk. According to spine surgeons we spoke with, MRI in the weight-bearing position is the only logical step to conduct as it gives important feedback on the soft tissue that cannot be obtained by other modalities.
Fenske: What were the most notable challenges in the development of this system and how did you overcome them?
van Kemenade: WB-MRI poses two important challenges—movement and artifacts. Patients who have severe back pain often cannot stand for a long period of time. Thanks to the eXP platform (speed plus image quality) and the clinical feedback from two important reference sites (Sports Klinik Stuttgart, Germany and Parker Institute, Copenhagen, Denmark), we were able to develop a “10-minute weight-bearing imaging protocol” to comply with these requisites.
In short, we position the patient at about 85 degrees, which, from a biomechanical point, gives an almost full WB effect, but at the same time, stabilizes the patient so there is less movement. As the main target is biomechanics, a high-res, isotropic 3D scan of the spine is first performed and then followed by a T2 weighted scan—all in about 10 minutes.
The 3D gives the possibility to perform subsequent reconstruction in any desired plane to evaluate biomechanics and the T2 is pathology oriented. After this, the patient table is rotated and the exam is completed with “normal” or standard imaging protocol.
Fenske: Will you look to adapt the technology for other imaging applications? Do you have any specific targets in mind?
van Kemenade: For the WB-MRI application, there is an interest for specific pathologies of the female pelvis where WB MRI could give an added diagnostic value. We have some sites that are looking into this; the first results are very promising. We are also experimenting with real-time MRI or MRI fluoroscopy as our system and coil design has taken this application into consideration from the beginning. Also hearing initial positive feedback in particular from sites specialized in sports medicine.
Fenske: What has been the industry response to this technology?
van Kemenade: Regarding the industry, there will always be a place for smaller companies that address particular clinical needs. Large companies work in a different economical framework; they have to sell large quantities to make it economically interesting for them. Just think of the costs of product introductions (marketing, training, roadshows, etc.) in a large, worldwide organization. For a company the size of Esaote, we are big enough to sustain the MRI R&D costs but small enough to be profitable with smaller sales numbers. MSK MRI is a very big chunk of the total MRI workload and, next to the particular WB-MRI application, we simply offer systems that can do excellent MSK-MRI imaging with a cost/benefit ratio that is clearly better than traditional MRI.
Fenske: Where is the imaging industry headed? What do you foresee coming down the pipeline five to ten years out?
van Kemenade: My personal vision is that, little by little, MRI will head into the x-ray direction where there are different systems for different needs, from a simple C-arm to sophisticated bi-plane angio/cardio systems. No doctor will consider examining a broken wrist on a bi-plane cardio x-ray. Even if this was possible, this would be a clear waste of money and resources. Now, why is the same principle not applied in MRI? Clinical papers show that, for example, the diagnostic outcome for meniscal tear using a 1.5T and a dedicated system are the same. In the medical world, changing the mindset is a slow process but the cost constraints in medical imaging are clearly in our favor and will speed-up this process.
Fenske: Any other comments or thoughts you’d like to share?
van Kemenade: Over the last few years, dedicated MRI has definitely evolved, with a huge improvement in image quality and reduced scan times. Unfortunately, many radiologists still have the images they saw maybe five years ago in mind. Today, every time we show current images (DICOM) at congresses like RSNA or ECR, we always get feedback like, “I didn’t expect such good quality,” or “Are these made with your small systems?” Unfortunately, it takes time to get this message into the market. From this point of view, it would, of course, be nice to have the big marketing budget of a large multi-national.
Get a look at the G-Scan Brio.